

Cathepsin Z as a novel potential biomarker for osteoporosis
- PMID: 31278293
- PMCID: PMC6611782
- DOI: 10.1038/s41598-019-46068-0
Cathepsin Z as a novel potential biomarker for osteoporosis
Abstract
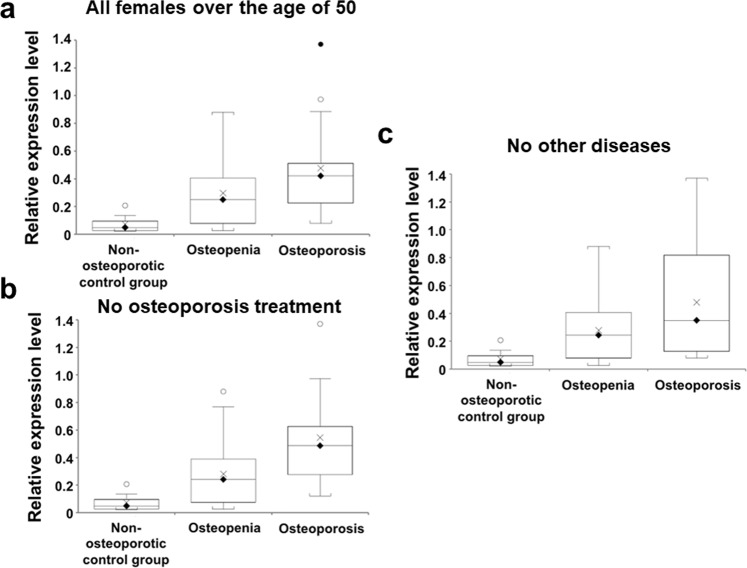
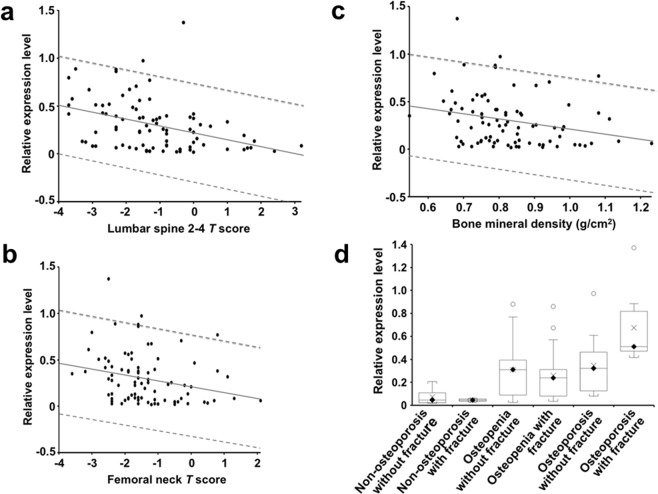
Osteoporosis, one of the most prevalent chronic ageing-related bone diseases, often goes undetected until the first fragility fracture occurs, causing patient suffering and cost to health/social care services. Osteoporosis arises from imbalanced activity of osteoclasts and osteoblasts. Since these cell lineages produce the protease, cathepsin Z, the aim of this study was to investigate whether altered cathepsin Z mRNA levels are associated with osteoporosis in clinical samples. Cathepsin Z mRNA in human peripheral blood mononuclear cells was significantly differentially-expressed among non-osteoporotic controls, osteopenia and osteoporosis patients (p < 0.0001) and in female osteoporosis patients over the age of 50 years (P = 0.0016). Cathepsin Z mRNA level strongly correlated with low bone mineral density (BMD) (g/cm2), lumbar spine L2-L4 and femoral neck (T-scores) (P = 0.0149, 0.0002 and 0.0139, respectively). Importantly, cathepsin Z mRNA was significantly associated with fragility fracture in osteoporosis patients (P = 0.0018). The levels of cathepsin Z mRNA were not significantly higher in patients with chronic inflammatory disorders in these two groups compared to those without (P = 0.774 and 0.666, respectively). ROC analysis showed that cathepsin Z mRNA has strong diagnostic value for osteoporosis and osteoporotic fracture. The results show for the first time that cathepsin Z could be a future diagnostic biomarker for osteoporosis including female osteoporosis patients over the age of 50 years.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
