

Silent Changes in Sleep Quality Following Mandibular Setback Surgery in Patients with Skeletal Class III Malocclusion: A Prospective Study
- PMID: 31278306
- PMCID: PMC6611882
- DOI: 10.1038/s41598-019-46166-z
Silent Changes in Sleep Quality Following Mandibular Setback Surgery in Patients with Skeletal Class III Malocclusion: A Prospective Study
Abstract
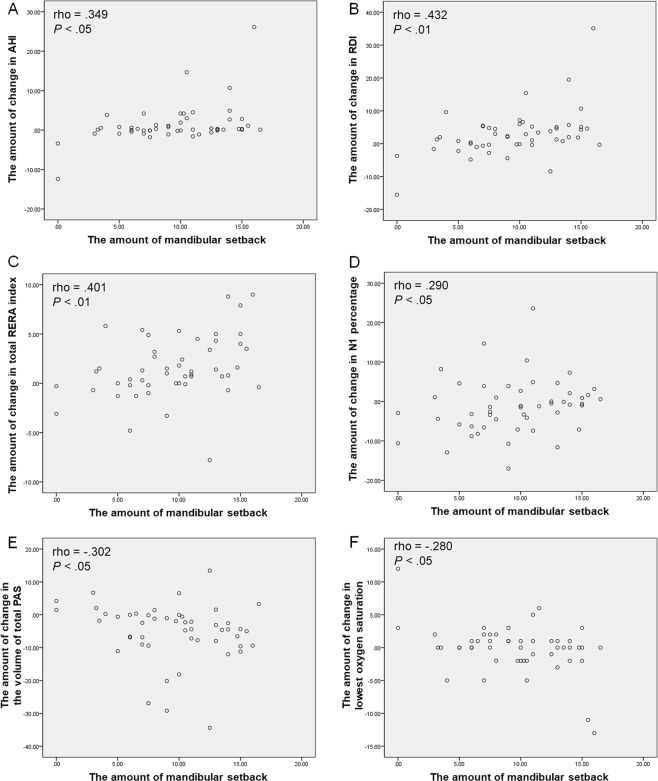
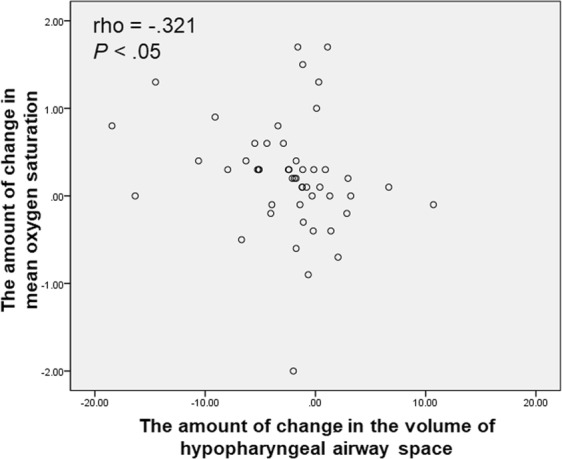
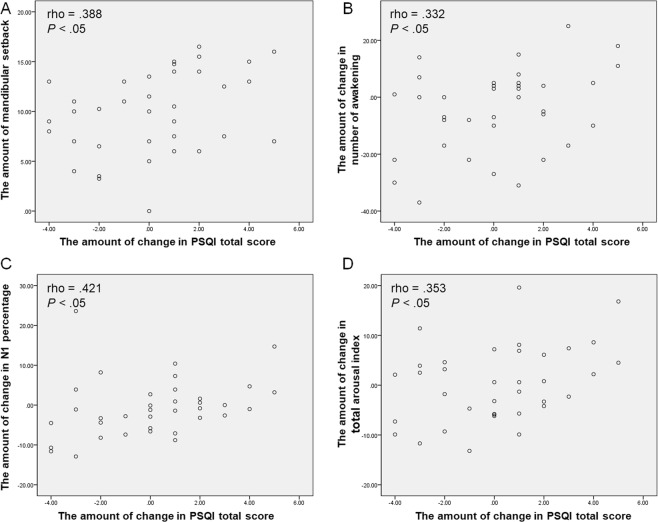
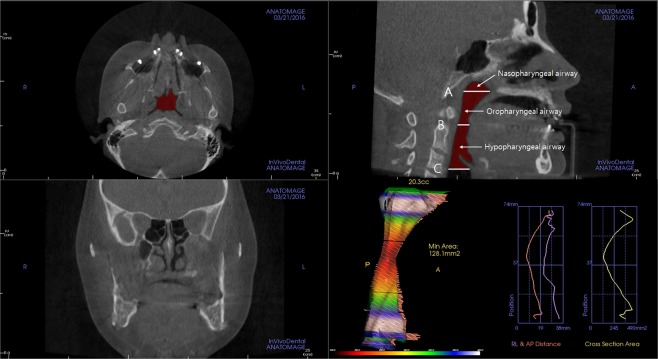
Mandibular setback surgery (MSS) for skeletal class III patients can result in a relative reduction of pharyngeal airway space (PAS). Consequently, there is a possibility of the decline of sleep quality after surgery. We investigated changes in sleep quality measured by overnight polysomnography (PSG) and the three-dimensional (3D) volumes of PAS following MSS with or without Le Fort I osteotomy (LF I) in class III patients (N = 53). Overnight PSG and cone beam computed tomography were conducted at preoperative stage (T0) and postoperative 3 months (T1). Measurements of PAS volumes were performed, and the subjective symptoms of sleep were evaluated by self-questionnaires. There were significant increases in respiratory disturbance index (RDI) and total respiratory effort-related arousal (RERA) index during T0-T1. The 3D volumes of PAS showed significant decreases in the oropharyngeal airway, hypopharyngeal airway, and total airway spaces. No significant changes were observed in subjective symptoms of sleep. MSS with or without LF I for class III patients could worsen sleep quality by increasing sleep parameters such as the RDI and RERA in PSG, and reduce volumes of PAS at postoperative 3 months. Although subjective symptoms may not show significant changes, objective sleep quality in PSG might decrease after MSS.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Effects of bimaxillary orthognathic surgery on pharyngeal airway and respiratory function at sleep in patients with class III skeletal relationship.J Craniomaxillofac Surg. 2018 Apr;46(4):645-653. doi: 10.1016/j.jcms.2018.01.009. Epub 2018 Feb 2. J Craniomaxillofac Surg. 2018. PMID: 29496371
-
Effects of orthognathic surgery on pharyngeal airway and respiratory function during sleep in patients with mandibular prognathism.Int J Oral Maxillofac Surg. 2014 Sep;43(9):1082-90. doi: 10.1016/j.ijom.2014.06.010. Epub 2014 Jul 12. Int J Oral Maxillofac Surg. 2014. PMID: 25027545
-
Effects of surgical correction of class III malocclusion on the pharyngeal airway and its influence on sleep apnoea.Int J Oral Maxillofac Surg. 2016 Dec;45(12):1508-1512. doi: 10.1016/j.ijom.2016.09.002. Epub 2016 Sep 26. Int J Oral Maxillofac Surg. 2016. PMID: 27688168
-
Impacts of mandibular setback with or without maxillary advancement for class III skeletal correction on sleep-related respiratory parameters: A systematic review and meta-analysis.Orthod Craniofac Res. 2024 Dec;27(6):839-852. doi: 10.1111/ocr.12798. Epub 2024 Apr 25. Orthod Craniofac Res. 2024. PMID: 38661057
-
Effect of orthognathic surgery on the posterior airway space (PAS).Ann Acad Med Singap. 2008 Aug;37(8):677-82. Ann Acad Med Singap. 2008. PMID: 18797561 Review.
Cited by
-
Changes in the pharyngeal airway after different orthognathic procedures for correction of class III dysplasia.Maxillofac Plast Reconstr Surg. 2022 Jun 9;44(1):23. doi: 10.1186/s40902-022-00352-8. Maxillofac Plast Reconstr Surg. 2022. PMID: 35678935 Free PMC article.
-
Why most patients do not exhibit obstructive sleep apnea after mandibular setback surgery?Maxillofac Plast Reconstr Surg. 2020 Mar 17;42(1):7. doi: 10.1186/s40902-020-00250-x. eCollection 2020 Dec. Maxillofac Plast Reconstr Surg. 2020. PMID: 32206666 Free PMC article. Review.
-
Effects of mandibular setback surgery using the surgery-first approach versus conventional orthognathic approach on upper airway change and sleep quality.Head Face Med. 2025 May 10;21(1):37. doi: 10.1186/s13005-025-00517-6. Head Face Med. 2025. PMID: 40349082 Free PMC article.
-
A prospective cohort study on effects of mandibular setback with or without maxillary advancement for skeletal class III malocclusion on sleep-related respiratory parameters.Sleep Breath. 2025 Apr 30;29(2):174. doi: 10.1007/s11325-025-03347-7. Sleep Breath. 2025. PMID: 40304815 Free PMC article.
References
-
- Fernandez-Ferrer L, Montiel-Company JM, Pinho T, Almerich-Silla JM, Bellot-Arcis C. Effects of mandibular setback surgery on upper airway dimensions and their influence on obstructive sleep apnoea - a systematic review. J. Craniomaxillofac. Surg. 2015;43:248–253. doi: 10.1016/j.jcms.2014.11.017. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
