

Impact of chronic migraine attacks and their severity on the endogenous μ-opioid neurotransmission in the limbic system
- PMID: 31279240
- PMCID: PMC6612052
- DOI: 10.1016/j.nicl.2019.101905
Impact of chronic migraine attacks and their severity on the endogenous μ-opioid neurotransmission in the limbic system
Abstract
Objective: To evaluate, in vivo, the impact of ongoing chronic migraine (CM) attacks on the endogenous μ-opioid neurotransmission.
Background: CM is associated with cognitive-emotional dysfunction. CM is commonly associated with frequent acute medication use, including opioids.
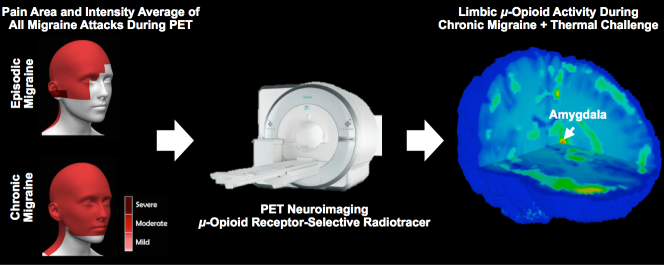
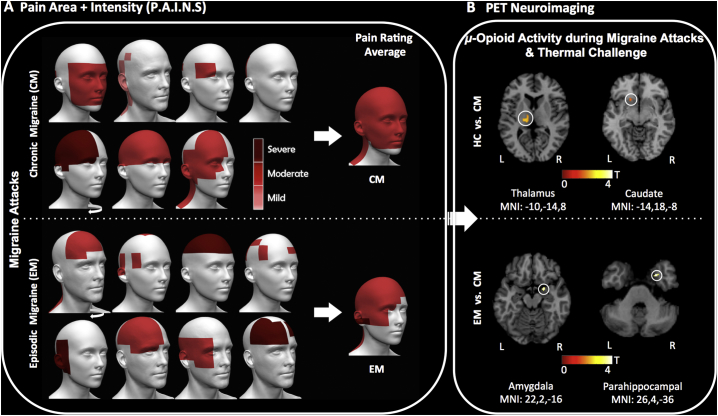
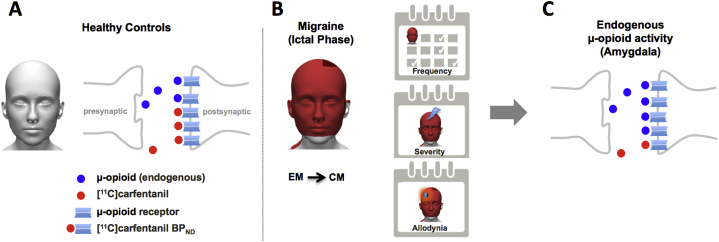
Methods: We scanned 15 migraine patients during the spontaneous headache attack (ictal phase): 7 individuals with CM and 8 with episodic migraine (EM), as well as 7 healthy controls (HC), using positron emission tomography (PET) with the selective μ-opioid receptor (μOR) radiotracer [11C]carfentanil. Migraineurs were scanned in two paradigms, one with thermal pain threshold challenge applied to the site of the headache, and one without thermal challenge. Multivariable analysis was performed between the μ-opioid receptor availability and the clinical data.
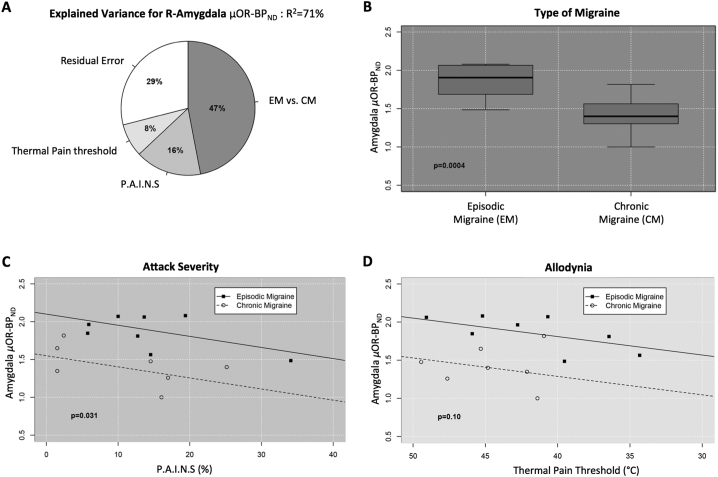
Results: μOR availability, measured with [11C]carfentanil nondisplaceable binding potential (BPND), in the left thalamus (P-value = 0.005) and left caudate (P-value = 0.003) were decreased in CM patients with thermal pain threshold during the ictal phase relative to HC. Lower μOR BPND in the right parahippocampal region (P-value = 0.001) and right amygdala (P-value = 0.002) were seen in CM relative to EM patients. Lower μOR BPND values indicate either a decrease in μOR concentration or an increase in endogenous μ-opioid release in CM patients. In the right amygdala, 71% of the overall variance in μOR BPND levels was explained by the type of migraine (CM vs. EM: partial-R2 = 0.47, P-value<0.001, Cohen's effect size d = 2.6SD), the severity of the attack (pain area and intensity number summation [P.A.I.N.S.]: partial-R2 = 0.16, P-value = 0.031), and the thermal pain threshold (allodynia: partial-R2 = 0.08).
Conclusions: Increased endogenous μ-opioid receptor-mediated neurotransmission is seen in the limbic system of CM patients, especially in right amygdala, which is highly modulated by the attack frequency, pain severity, and sensitivity. This study demonstrates for the first time the negative impact of chronification and exacerbation of headache attacks on the endogenous μ-opioid mechanisms of migraine patients. ClinicalTrials.gov identifier: NCT03004313.
Keywords: Central pain; MRI; Migraine; Opioid; PET; Thermal pain threshold.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Dopamine D2/D3 imbalance during migraine attack and allodynia in vivo.Neurology. 2017 Apr 25;88(17):1634-1641. doi: 10.1212/WNL.0000000000003861. Epub 2017 Mar 29. Neurology. 2017. PMID: 28356463 Free PMC article.
-
3D-neuronavigation in vivo through a patient's brain during a spontaneous migraine headache.J Vis Exp. 2014 Jun 2;(88):50682. doi: 10.3791/50682. J Vis Exp. 2014. PMID: 24962460 Free PMC article.
-
Classifying migraine using PET compressive big data analytics of brain's μ-opioid and D2/D3 dopamine neurotransmission.Front Pharmacol. 2023 Jun 13;14:1173596. doi: 10.3389/fphar.2023.1173596. eCollection 2023. Front Pharmacol. 2023. PMID: 37383727 Free PMC article.
-
Migraine and the Mu-opioidergic system-Can we directly modulate it? Evidence from neuroimaging studies.Curr Pain Headache Rep. 2014 Jul;18(7):429. doi: 10.1007/s11916-014-0429-0. Curr Pain Headache Rep. 2014. PMID: 24842566 Free PMC article. Review.
-
Neural Plasticity in Migraine Chronification.Eur J Neurosci. 2025 Jan;61(2):e70007. doi: 10.1111/ejn.70007. Eur J Neurosci. 2025. PMID: 39854038 Review.
Cited by
-
Endogenous opioid systems alterations in pain and opioid use disorder.Front Syst Neurosci. 2022 Oct 19;16:1014768. doi: 10.3389/fnsys.2022.1014768. eCollection 2022. Front Syst Neurosci. 2022. PMID: 36341476 Free PMC article. Review.
-
Pain Management for Dental Medicine in 2021: Opioids, Coronavirus and Beyond.J Pain Res. 2021 May 24;14:1371-1387. doi: 10.2147/JPR.S319373. eCollection 2021. J Pain Res. 2021. PMID: 34079355 Free PMC article.
-
Is There Any MRI Pattern That Discriminates Female From Male Migraine Patients?Front Neurol. 2019 Sep 6;10:961. doi: 10.3389/fneur.2019.00961. eCollection 2019. Front Neurol. 2019. PMID: 31551917 Free PMC article. Review.
-
Migraine in men.J Headache Pain. 2025 Jan 3;26(1):3. doi: 10.1186/s10194-024-01936-7. J Headache Pain. 2025. PMID: 39754046 Free PMC article. Review.
-
µ-Opioid Activity in Chronic TMD Pain Is Associated with COMT Polymorphism.J Dent Res. 2019 Nov;98(12):1324-1331. doi: 10.1177/0022034519871938. Epub 2019 Sep 6. J Dent Res. 2019. PMID: 31490699 Free PMC article.
References
-
- Benatto M.T., Florencio L.L., Carvalho G.F. Cutaneous allodynia is more frequent in chronic migraine, and its presence and severity seems to be more associated with the duration of the disease. Arq. Neuropsiquiatr. 2017;75:153–159. - PubMed
-
- Bigal M.E., Serrano D., Buse D., Scher A., Stewart W.F., Lipton R.B. Acute migraine medications and evolution from episodic to chronic migraine: a longitudinal population-based study. Headache. 2008;48:1157–1168. - PubMed
-
- Bigal M.E., Borucho S., Serrano D., Lipton R.B. The acute treatment of episodic and chronic migraine in the USA. Cephalalgia. 2009;29:891–897. - PubMed
-
- Brett M, Anton, JL, Valabrague, R, Poline, JB. Region of interest analysis using an SPM toolbox for SPM 99. NeuroImage;16:497.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
