

Comparison of two continuous non-invasive haemodynamic monitoring techniques in the perioperative setting
- PMID: 31281214
- PMCID: PMC6586383
- DOI: 10.6001/actamedica.v26i1.3953
Comparison of two continuous non-invasive haemodynamic monitoring techniques in the perioperative setting
Abstract
Background: The aim of the study was to identify the accuracy of and agreement between two non-invasive haemodynamic monitoring techniques in the perioperative setting - thoracic electrical bioimpedance (TEB) and Edwards Lifesciences ClearSight system (CS).
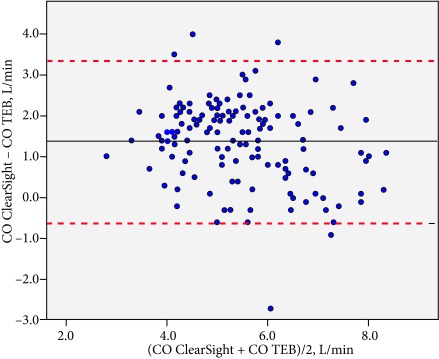
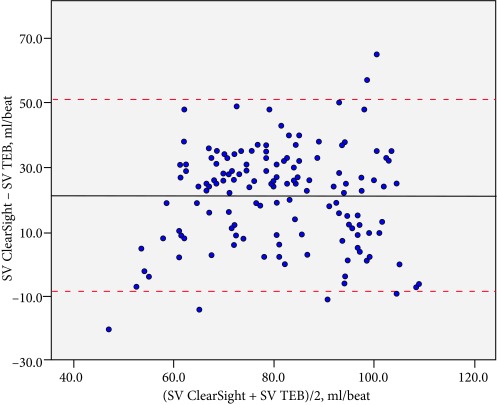
Materials and methods: The study included ten patients. Parametric quantitative data were expressed as mean ± SD. The Shapiro-Wilk test was used to test the normality of the distributions. A linear regression model was used to measure the strength of the linear relationship between TEB and CS. Bland-Altman analysis was performed to assess the mean difference, precision, and the limits of agreements (LOA). The Critchley and Critchley method was used to calculate the percentage error (PE), and if <30%, it was considered clinically acceptable.
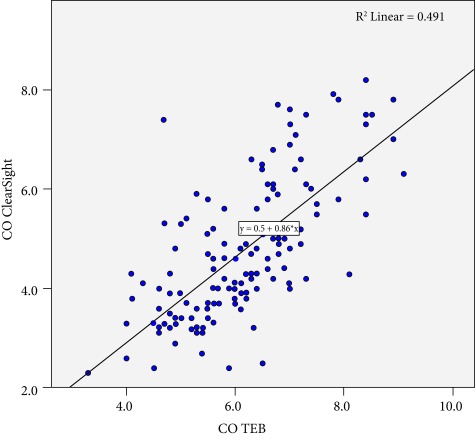
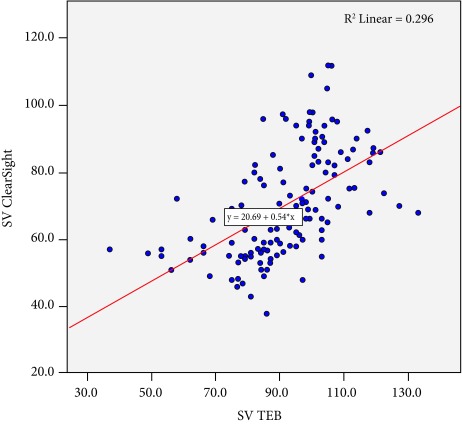
Results: Ten patients were involved in our study. The mean cardiac output (CO) with TEB was 6.15 ± 1.14 L/min vs. 4.78 ± 1.40 L/min with CS (p < 0.01). The relationship was significant (n = 144; r 2 = 0.7; p < 0.01). The mean bias, LOA, and PE were 1.37 ± 1.01 L/min, 3.35 L/min and -0.61 L/min and 36.22%, respectively. The mean stroke volume index (SVI) with TEB was 48.64 ± 9.8 ml/beat/m2 vs. 37.12 ± 9.14 ml/beat/m2 with CS (p < 0.01). The relationship was significant (n = 144; r 2 = 0.65; p < 0.01). The mean bias, LOA, and PE were 11.52 ± 7.92 ml/beat/m2, 27.04 ml/beat/m2 and -4 ml/beat/m2 and 36.19%.
Conclusions: The two methods of non-invasive haemodynamic monitoring are not compatible in the perioperative setting. However, the CS system has more advantages in terms of continuity and simplicity of monitoring, while measurements of TEB are interrupted by electrocautery.
SantraukaĮvadas. Tyrimo tikslas – nustatyti dviejų neinvazinių hemodinamikos monitoravimo technikų tikslumą ir suderinamumą, lyginant bioimpedansą ir Edwards Lifesciences ClearSight sistemą.Tyrimo medžiaga ir metodai. Tyrime dalyvavo 10 pacientų. Kiekybiniai duomenys pateikti kaip aritmetiniai vidurkiai su standartiniu nuokrypiu. Skirstinio normalumui patikrinti naudotas Šapiro-Vilko testas. Tarpusavio ryšio stiprumui tarp bioimpedanso ir ClearSight įvertinti pasitelkta linijinė regresinė analizė. Bland-Altman analizė panaudota nustatant vidutinį skirtumą, tikslumą ir sutarties ribas. Critchley ir Critchley metodas buvo naudojamas apskaičiuojant procentinę paklaidą. Jei paklaida mažesnė nei 30 %, laikyta, kad ji kliniškai priimtina.Rezultatai. Vidutinis širdies minutinis tūris išmatuotas bioimpedansu; 6,15 ± 1,14 l/min., CS 4,78 ± 1,40 l/min. (p < 0,01). Nustatytas vidutinio stiprumo ryšys tarp minutinio širdies tūrio matavimų (n = 144; r 2 = 0,7; p < 0,01). Vidutinis skirtumas – 1,37 ± 1,01 l/min., sutarties ribos nuo 3,35 l/min. iki –0,61 l/min., paklaida – 36,22 %. Vidutinis sitolinio tūrio indeksas išmatuotas bioimpedansu: 48,64 ± 9,8 ml/susitraukimui/m2 ir CS 7,12 ± 9,14 ml/susitraukimui/m2 (p < 0,01). Nustatytas vidutinio stiprumo ryšys tarp sistolinio tūrio indekso matavimų (n = 144; r2 = 0,65; p < 0,01). Vidutinis skirtumas – 11,52 ± 7,92 ml/susitraukimui/m2, sutarties ribos: 27,04 ml/susitraukimui/m2 –4 ml/susitraukimui/m2 ir paklaida 36,19 %.Išvados. Šie neinvaziniai hemodinamikos stebėjimo metodai perioperaciniu laikotarpiu yra nesuderinami. Tačiau ClearSight pranašesnis dėl metodo paprastumo ir tęstinumo, o bioimpedanso matavimams įtaką darė elektrinio peilio naudojimas.Raktažodžiai: hemodinamikos stebėsena, minutinis širdies tūris, neinvazinis, intraoperacinis, pulso bangos analizė, bioimpedansas.
Keywords: bioimpedance; cardiac output; haemodynamic monitoring; intraoperative; non-invasive; pulse wave analysis.
Figures
Similar articles
-
The accuracy of bioimpedance cardiography in the measurement of cardiac output in comparison with thermodilution method.Acta Anaesthesiol Sin. 1996 Jun;34(2):55-9. Acta Anaesthesiol Sin. 1996. PMID: 9084523
-
Continuous non-invasive measurement of stroke volume and cardiac index in infants and children: comparison of Impedance Cardiography NICaS® vs CardioQ® method.Clin Ter. 2018 May-Jun;169(3):e110-e113. doi: 10.7417/T.2018.2064. Clin Ter. 2018. PMID: 29938742
-
Perioperative non-invasive versus semi-invasive cardiac index monitoring in patients with bariatric surgery - a prospective observational study.BMC Anesthesiol. 2020 Aug 10;20(1):196. doi: 10.1186/s12871-020-01110-x. BMC Anesthesiol. 2020. PMID: 32778047 Free PMC article. Clinical Trial.
-
Continuous noninvasive pulse wave analysis using finger cuff technologies for arterial blood pressure and cardiac output monitoring in perioperative and intensive care medicine: a systematic review and meta-analysis.Br J Anaesth. 2020 Jul;125(1):25-37. doi: 10.1016/j.bja.2020.03.013. Epub 2020 May 29. Br J Anaesth. 2020. PMID: 32475686
-
Accuracy and precision of non-invasive cardiac output monitoring by electrical cardiometry: a systematic review and meta-analysis.J Clin Monit Comput. 2020 Jun;34(3):433-460. doi: 10.1007/s10877-019-00330-y. Epub 2019 Jun 7. J Clin Monit Comput. 2020. PMID: 31175501 Free PMC article.
Cited by
-
Non invasive hemodynamic monitoring for fluids and blood resuscitation during placenta praevia accreta cesarean delivery: a retrospective observational study.J Anesth Analg Crit Care. 2022 Dec 27;2(1):54. doi: 10.1186/s44158-022-00083-2. J Anesth Analg Crit Care. 2022. PMID: 37386677 Free PMC article.
References
-
- Association of Anaesthetists of Great Britain & Ireland. Checking Anaesthetic Equipment 2012. AAGBI Safety Guideline. London, 2012. - PubMed
-
- Clement RP, Vos JJ, Scheeren TWL. Minimally invasive cardiac output technologies in the ICU: putting it all together. Curr Opin Crit Care. 2017. August; 23(4): 302–9. - PubMed
LinkOut - more resources
Full Text Sources