

Reevaluating the Role of Corticosteroids in Septic Shock: An Updated Meta-Analysis of Randomized Controlled Trials
- PMID: 31281831
- PMCID: PMC6590573
- DOI: 10.1155/2019/3175047
Reevaluating the Role of Corticosteroids in Septic Shock: An Updated Meta-Analysis of Randomized Controlled Trials
Abstract
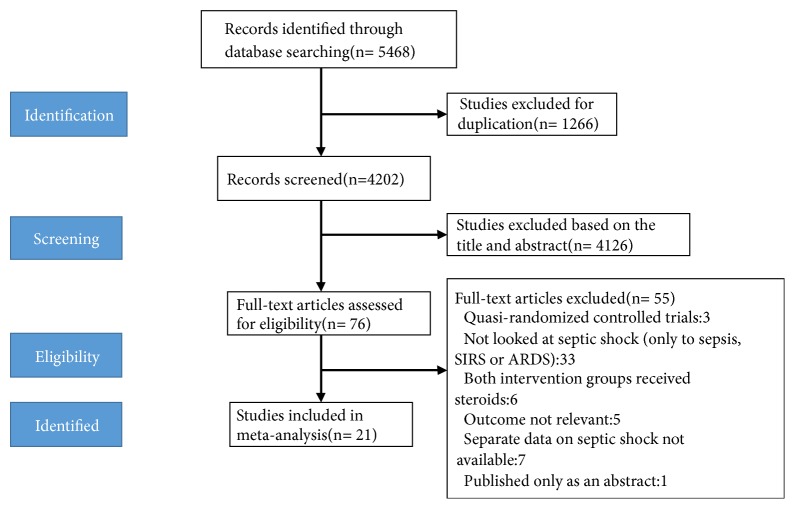
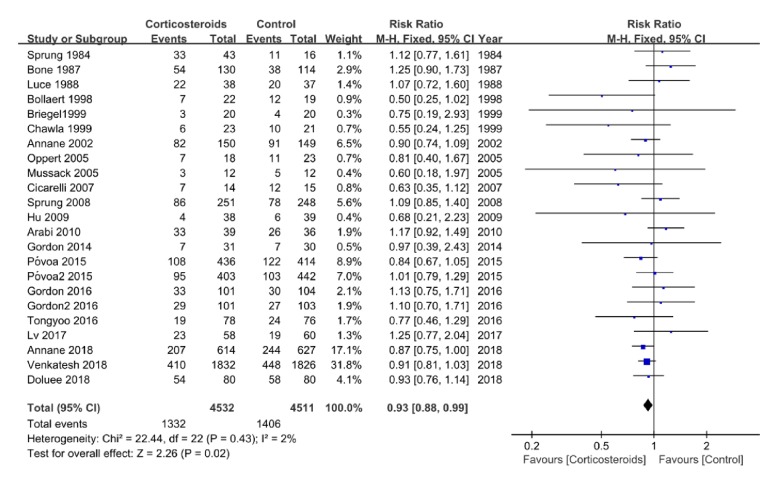
What Is Known and Objective. To reevaluate the benefits and risks of corticosteroid treatment in adult patients with septic shock. Methods. This study was performed based on PRISMA guidelines. Randomized controlled trials (RCTs) of corticosteroids versus placebo were retrieved from PubMed, MEDLINE, EMBASE, Web of Science, the Cochrane Central RCTs, and ClinicalTrials.gov from January 1980 to April 2018. We also conducted a trial sequential analysis to indicate the possibility of type I or II errors and calculate the information size. Grading of Recommendations, Assessment, Development and Evaluation approach (GRADE) was applying to assess the certainty of evidence at the primary outcome level. Results. Twenty-one RCTs were identified and analyzed. Patients treated with corticosteroid had a 7% reduction in relative risk in 28-day all-cause mortality compared to controls (RR 0.93, 95% CI 0.88 to 0.99). However, there were no significant differences for the intensive care unit (ICU) mortality (RR 0.97, 95% CI 0.86 to 1.09) or in-hospital mortality (RR 1.01, 95% CI 0.92 to 1.11). Corticosteroids shortened the length of ICU stay by 1.04 days (RR -1.04, 95% CI -1.72 to -0.36) and the length of hospital stay by 2.49 days (RR -2.49, 95% CI -4.96 to -0.02). Corticosteroids increased the risk of hyperglycemia (RR 1.11, 95% CI 1.06 to 1.16) but not gastroduodenal bleeding (RR 1.06, 95% CI 0.82 to 1.37) or superinfection (RR 1.04, 95% CI 0.94 to 1.15). However, some date on secondary outcomes were unavailable because they were not measured or not reported in the included studies which may cause a lack of power or selective outcome reporting. The information size was calculated at 10044 patients. Trial sequential analysis showed that the meta-analysis was conclusive and the risk of type 2 error was minimal. What Is New and Conclusion. Corticosteroids are likely to be effective in reducing 28-day mortality and attenuating septic shock without increasing the rate of life-threatening complications. TSA showed that the risk of type II error in this meta-analysis was minimal and the result was conclusive.
Figures



Similar articles
-
Association of Corticosteroid Treatment With Outcomes in Adult Patients With Sepsis: A Systematic Review and Meta-analysis.JAMA Intern Med. 2019 Feb 1;179(2):213-223. doi: 10.1001/jamainternmed.2018.5849. JAMA Intern Med. 2019. PMID: 30575845 Free PMC article.
-
The Effectiveness and Safety of Corticosteroids Therapy in Adult Critical Ill Patients With Septic Shock: A Meta-Analysis of Randomized Controlled Trials.Shock. 2019 Aug;52(2):198-207. doi: 10.1097/SHK.0000000000001202. Shock. 2019. PMID: 29889815
-
Corticosteroids for Managing Pediatric Sepsis and Septic Shock: A Systematic Review and Meta-analysis.Pediatr Infect Dis J. 2025 Jan 1;44(1):74-82. doi: 10.1097/INF.0000000000004551. Epub 2024 Sep 25. Pediatr Infect Dis J. 2025. PMID: 39348497
-
Effect of Low-Dose Hydrocortisone Therapy in Adult Patients With Septic Shock: A Meta-Analysis With Trial Sequential Analysis of Randomized Controlled Trials.J Intensive Care Med. 2020 Oct;35(10):971-983. doi: 10.1177/0885066618803062. Epub 2018 Oct 1. J Intensive Care Med. 2020. PMID: 30270720
-
Corticosteroids for Treating Sepsis in Adult Patients: A Systematic Review and Meta-Analysis.Front Immunol. 2021 Aug 16;12:709155. doi: 10.3389/fimmu.2021.709155. eCollection 2021. Front Immunol. 2021. PMID: 34484209 Free PMC article.
Cited by
-
Neuroendocrine Modulation of the Immune Response after Trauma and Sepsis: Does It Influence Outcome?J Clin Med. 2020 Jul 18;9(7):2287. doi: 10.3390/jcm9072287. J Clin Med. 2020. PMID: 32708472 Free PMC article. Review.
-
Cytokine Storm in Novel Coronavirus Disease (COVID-19): Expert Management Considerations.Indian J Crit Care Med. 2020 Jun;24(6):429-434. doi: 10.5005/jp-journals-10071-23415. Indian J Crit Care Med. 2020. PMID: 32863636 Free PMC article.
-
Effectiveness of corticosteroids in patients with sepsis or septic shock using the new third international consensus definitions (Sepsis-3): A retrospective observational study.PLoS One. 2020 Dec 3;15(12):e0243149. doi: 10.1371/journal.pone.0243149. eCollection 2020. PLoS One. 2020. PMID: 33270762 Free PMC article.
-
Surviving Sepsis Campaign: guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19).Intensive Care Med. 2020 May;46(5):854-887. doi: 10.1007/s00134-020-06022-5. Epub 2020 Mar 28. Intensive Care Med. 2020. PMID: 32222812 Free PMC article.
-
Expert consensus on the glycemic management of critically ill patients.J Intensive Med. 2022 Jul 8;2(3):131-145. doi: 10.1016/j.jointm.2022.06.001. eCollection 2022 Jul. J Intensive Med. 2022. PMID: 36789019 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
