

Plasma Proinflammatory Cytokines Are Markers of Disease Severity and Bacterial Burden in Pulmonary Tuberculosis
- PMID: 31281858
- PMCID: PMC6602384
- DOI: 10.1093/ofid/ofz257
Plasma Proinflammatory Cytokines Are Markers of Disease Severity and Bacterial Burden in Pulmonary Tuberculosis
Abstract
Background: Type 1, type 17, and other proinflammatory cytokines are important in host immunity to tuberculosis (TB) in animal models. However, their role in human immunity to TB is not completely understood.
Methods: To examine the association of proinflammatory cytokines with pulmonary TB (PTB), we examined the plasma levels of type 1 (interferon [IFN]γ and tumor necrosis factor [TNF]α), type 17 (interleukin [IL]-17A and IL-17F), and other proinflammatory (IL-6, IL-12, and IL-1β) cytokines in individuals with PTB, latent TB (LTB), or healthy controls (HC).
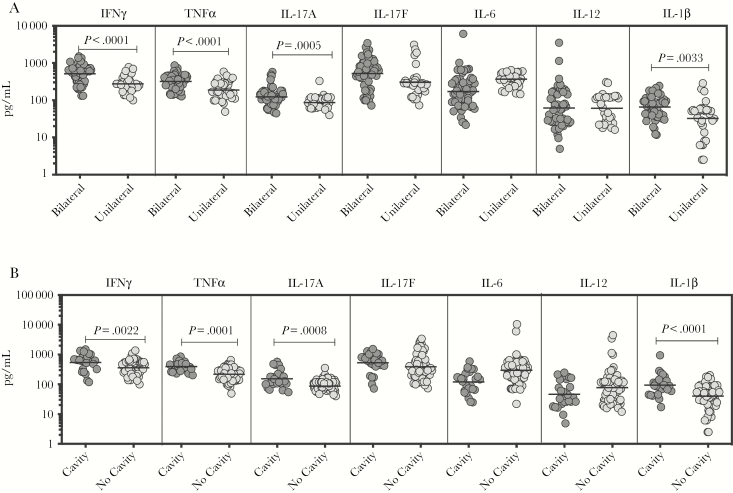
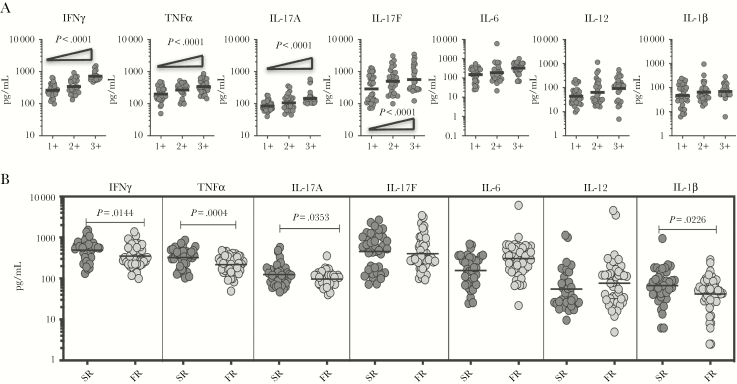
Results: Individuals with PTB exhibited significantly higher plasma levels of most of the above cytokines compared with LTB or HC individuals. Principal component analysis based on these cytokines could clearly distinguish PTB from both LTB or HC individuals. Pulmonary TB individuals with bilateral or cavitary disease exhibited significantly higher levels of IFNγ, TNFα, IL-17A, and IL-1β compared with those with unilateral or noncavitary disease. Pulmonary TB individuals also exhibited a significant positive relationship between IFNγ, TNFα, and IL-17A levels and bacterial burdens. In addition, PTB individuals with delayed culture conversion exhibited significantly higher levels of IFNγ, TNFα, IL-17A, and IL-1β at baseline. Finally, the plasma levels of all the cytokines examined were significantly reduced after successful chemotherapy.
Conclusions: Therefore, our data demonstrate that PTB is associated with heightened levels of plasma proinflammatory cytokines, which are reversed after chemotherapy. Our data also reveal that proinflammatory cytokines are markers of disease severity, bacterial burden, and delayed culture conversion in PTB.
Keywords: biomarkers; cytokines; tuberculosis.
Figures


References
-
- Pai M, Behr MA, Dowdy D, et al. Tuberculosis. Nat Rev Dis Primers 2016; 2:16076. - PubMed
-
- O’Garra A, Redford PS, McNab FW, et al. The immune response in tuberculosis. Annu Rev Immunol 2013; 31:475–527. - PubMed
-
- Casanova JL, Abel L. Genetic dissection of immunity to mycobacteria: the human model. Annu Rev Immunol 2002; 20:581–620. - PubMed
