

Representativeness of Randomized Clinical Trial Cohorts in End-stage Kidney Disease: A Meta-analysis
- PMID: 31282924
- PMCID: PMC6618769
- DOI: 10.1001/jamainternmed.2019.1501
Representativeness of Randomized Clinical Trial Cohorts in End-stage Kidney Disease: A Meta-analysis
Erratum in
-
Pervasive Errors Due to Duplicate Trial Cohorts.JAMA Intern Med. 2019 Oct 1;179(10):1448. doi: 10.1001/jamainternmed.2019.5040. JAMA Intern Med. 2019. PMID: 31589254 Free PMC article. No abstract available.
Abstract
Importance: Systematic differences between patients included in randomized clinical trials (RCTs) and the general patient population may influence the generalizability of RCT findings. Comprehensive national registries of patients with end-stage kidney disease who are undergoing dialysis provide a unique opportunity to compare trial and real-world patient cohorts.
Objective: To determine if participants in large, multicenter dialysis trials were similar to the general population undergoing dialysis in terms of age, comorbidities, and mortality rate.
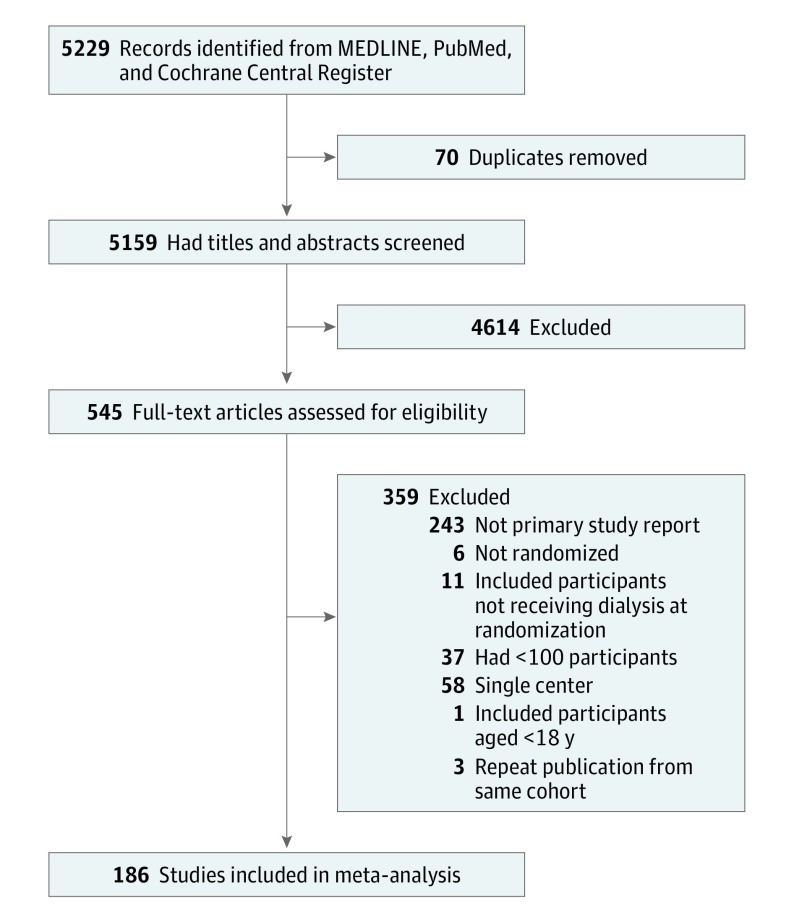
Data sources: MEDLINE, PubMed, and the Cochrane Central Register of Controlled Trials were systematically searched on January 6, 2017, for studies published from January 1, 2007, to December 31, 2016. Data sources were published manuscripts, supplementary material, and trial registration information. Data on the general population undergoing dialysis were derived from the US Renal Data System (USRDS). Data were analyzed from March 17 to July 22, 2018.
Study selection: Randomized clinical trials enrolling only participants undergoing dialysis for end-stage kidney disease with 100 or more adult participants from 2 or more sites.
Data extraction and synthesis: Abstract screening and data extraction were performed independently by 2 researchers. Data were pooled using a random-effects model.
Main outcomes and measures: The primary outcome was difference in mean age between the RCT and USRDS populations. Secondary outcomes included differences in mortality rate and comorbidities.
Results: The search identified 186 RCTs, enrolling 79 104 participants. Compared with the 2011 USRDS population, RCT participants were younger (mean age, 58.9 years; 95% CI, 58.3-59.5 years vs 61.2 years; P < .001), more likely to be male (58.9%; 95% CI, 57.6%-60.1% vs 55.7%; P < .001), and have coronary artery disease (26.9%; 95% CI, 22.2%-31.7% vs 17.7%; P < .001) and less likely to have diabetes (40.2%; 95% CI, 36.7%-43.6% vs 44.2%; P = .03) or heart failure (19.6%; 95% CI, 15.1%-24.0% vs 29.8%; P < .001). The mortality rate per 100 patient-years during trial participation was less than half that of the USRDS population (8.9; 95% CI, 7.8-10.0 vs 18.6; P < .001). The differences in age, mortality, and coronary artery disease remained when studies recruiting only from the United States were considered. Diabetes was more common in RCT participants from the United States than in the registry population.
Conclusions and relevance: Participants in large, multicenter RCTs of patients with end-stage kidney disease undergoing dialysis are younger, have a different pattern of comorbidities, and have a lower mortality rate than the general population of patients undergoing dialysis. This finding has implications for the generalization of trial results to the broader patient population and for future trial design.
Conflict of interest statement
Comment in
-
Disparities between trial cohorts and real-life patients.Nat Rev Nephrol. 2019 Nov;15(11):666-667. doi: 10.1038/s41581-019-0202-z. Nat Rev Nephrol. 2019. PMID: 31477914 No abstract available.
-
Studies Making Use of the Same Randomized Clinical Trial Cohorts.JAMA Intern Med. 2019 Oct 1;179(10):1446-1447. doi: 10.1001/jamainternmed.2019.4621. JAMA Intern Med. 2019. PMID: 31589263 No abstract available.
-
Studies Making Use of the Same Randomized Clinical Trial Cohorts-Reply.JAMA Intern Med. 2019 Oct 1;179(10):1447. doi: 10.1001/jamainternmed.2019.4624. JAMA Intern Med. 2019. PMID: 31589269 No abstract available.
References
-
- Golomb BA, Chan VT, Evans MA, Koperski S, White HL, Criqui MH. The older the better: are elderly study participants more non-representative? a cross-sectional analysis of clinical trial and observational study samples. BMJ Open. 2012;2(6):e000833. doi:10.1136/bmjopen-2012-000833 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
