

Neoadjuvant Three-Dimensional Conformal Radiotherapy for Resectable Hepatocellular Carcinoma With Portal Vein Tumor Thrombus: A Randomized, Open-Label, Multicenter Controlled Study
- PMID: 31283409
- PMCID: PMC6698917
- DOI: 10.1200/JCO.18.02184
Neoadjuvant Three-Dimensional Conformal Radiotherapy for Resectable Hepatocellular Carcinoma With Portal Vein Tumor Thrombus: A Randomized, Open-Label, Multicenter Controlled Study
Abstract
Purpose: To compare the survival outcomes of neoadjuvant three-dimensional conformal radiotherapy (RT) followed by hepatectomy with hepatectomy alone in patients with hepatocellular carcinoma (HCC) and portal vein tumor thrombus (PVTT).
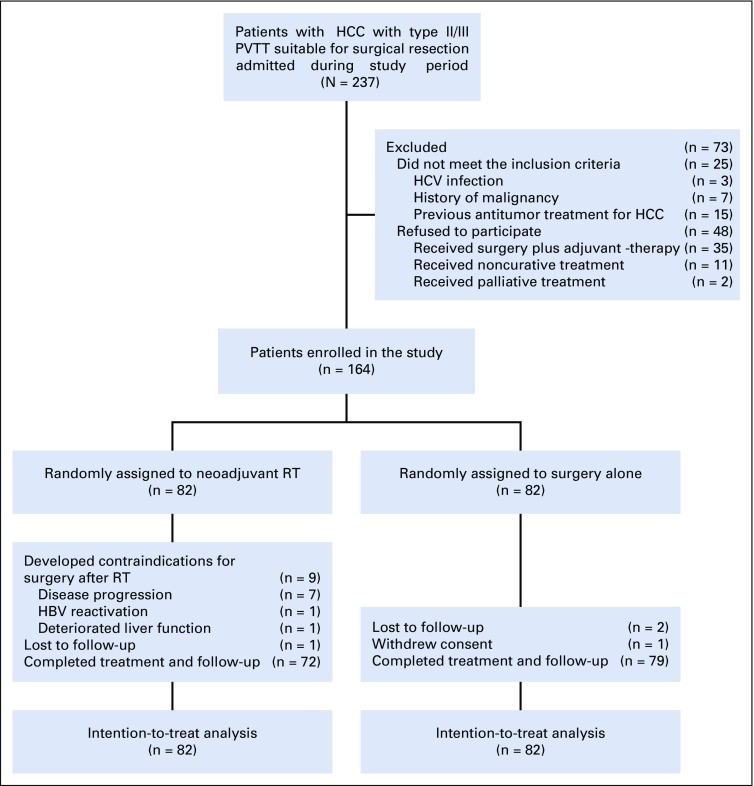
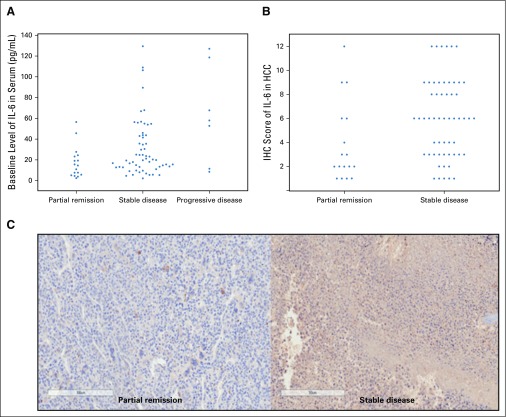
Patients and methods: A randomized, multicenter controlled study was conducted from January 2016 to December 2017 in patients with resectable HCC and PVTT. Patients were randomly assigned to receive neoadjuvant RT followed by hepatectomy (n = 82) or hepatectomy alone (n = 82). The modified Response Evaluation Criteria in Solid Tumors (mRECIST) guidelines were used to evaluate the therapeutic effects of RT. The primary end point was overall survival. The expression of interleukin-6 (IL-6) in patients' serum before RT and in surgical specimens was correlated with response to RT.
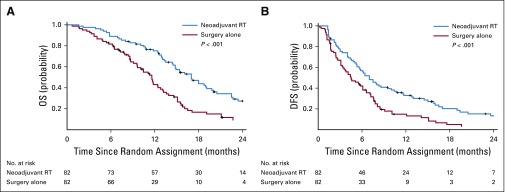
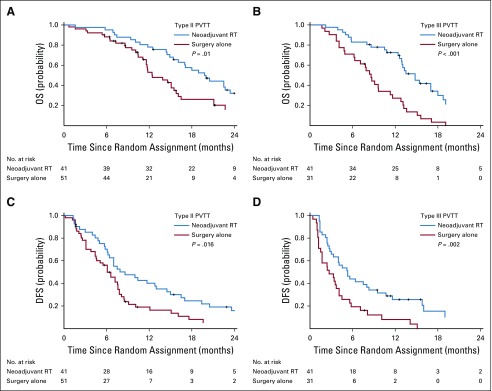
Results: In the neoadjuvant RT group, 17 patients (20.7%) had partial remission. The overall survival rates for the neoadjuvant RT group at 6, 12, 18, and 24 months were 89.0%, 75.2%, 43.9%, and 27.4%, respectively, compared with 81.7%, 43.1%, 16.7%, and 9.4% in the surgery-alone group (P < .001). The corresponding disease-free survival rates were 56.9%, 33.0%, 20.3%, and 13.3% versus 42.1%, 14.9%, 5.0%, and 3.3% (P < .001). On multivariable Cox regression analyses, neoadjuvant RT significantly reduced HCC-related mortality and HCC recurrence rates compared with surgery alone (hazard ratios, 0.35 [95% CI, 0.23 to 0.54; P < .001] and 0.45 [95% CI, 0.31 to 0.64; P < .001]). Increased expressions of IL-6 in pre-RT serum and tumor tissues were significantly associated with resistance to RT.
Conclusion: For patients with resectable HCC and PVTT, neoadjuvant RT provided significantly better postoperative survival outcomes than surgery alone. IL-6 may predict response to RT in these patients.
Figures
Comment in
-
Neoadjuvant radiotherapy improves hepatectomy survival.Lancet Oncol. 2019 Aug;20(8):e403. doi: 10.1016/S1470-2045(19)30457-7. Epub 2019 Jul 18. Lancet Oncol. 2019. PMID: 31327738 No abstract available.
-
Gastrointestinal Cancers: Moving the Needle for Rectal, Gastroesophageal, Pancreaticobiliary, and Liver Cancers.Int J Radiat Oncol Biol Phys. 2020 Mar 15;106(4):653-662. doi: 10.1016/j.ijrobp.2019.12.011. Int J Radiat Oncol Biol Phys. 2020. PMID: 32092335 No abstract available.
References
-
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. - PubMed
-
- European Association for the Study of the Liver: EASL clinical practice guidelines: Management of hepatocellular carcinoma. J Hepatol 69:182-236, 2018 [Erratum: J Hepatol 70:817, 2019] - PubMed
-
- Shuqun C, Mengchao W, Han C, et al. Tumor thrombus types influence the prognosis of hepatocellular carcinoma with the tumor thrombi in the portal vein. Hepatogastroenterology. 2007;54:499–502. - PubMed
-
- Sakata H, Konishi M, Ryu M, et al. Prognostic factors for hepatocellular carcinoma presenting with macroscopic portal vein tumor thrombus. Hepatogastroenterology. 2004;51:1575–1580. - PubMed
-
- Le Treut YP, Hardwigsen J, Ananian P, et al. Resection of hepatocellular carcinoma with tumor thrombus in the major vasculature. A European case-control series. J Gastrointest Surg. 2006;10:855–862. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
