

MRI of Tumors and Tumor Mimics in the Female Pelvis: Anatomic Pelvic Space-based Approach
- PMID: 31283453
- PMCID: PMC6677288
- DOI: 10.1148/rg.2019180173
MRI of Tumors and Tumor Mimics in the Female Pelvis: Anatomic Pelvic Space-based Approach
Abstract
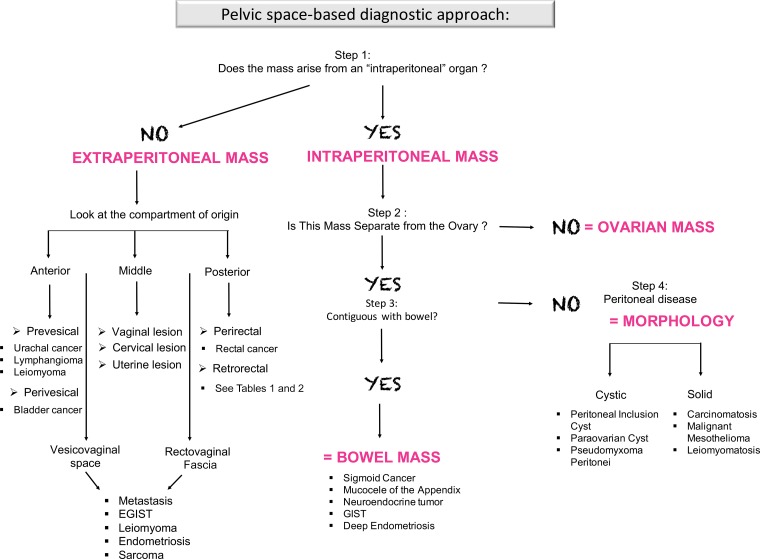
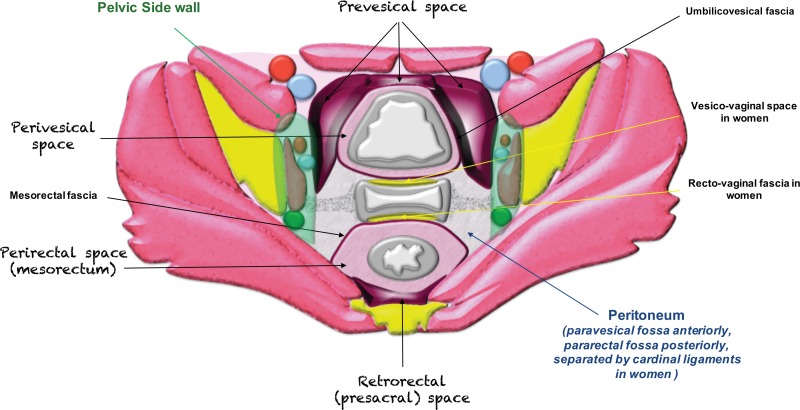
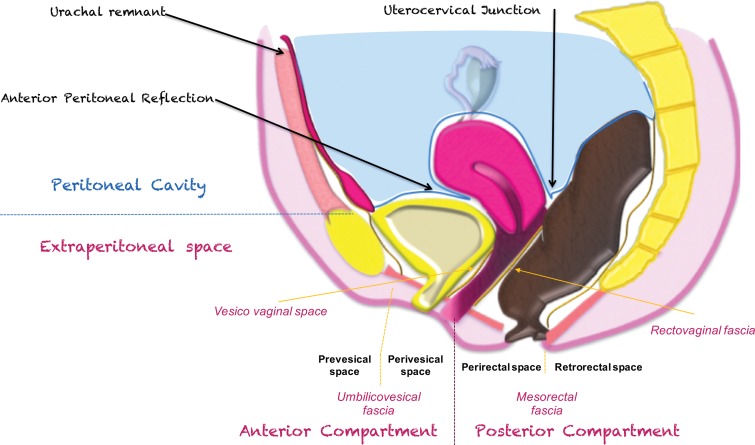
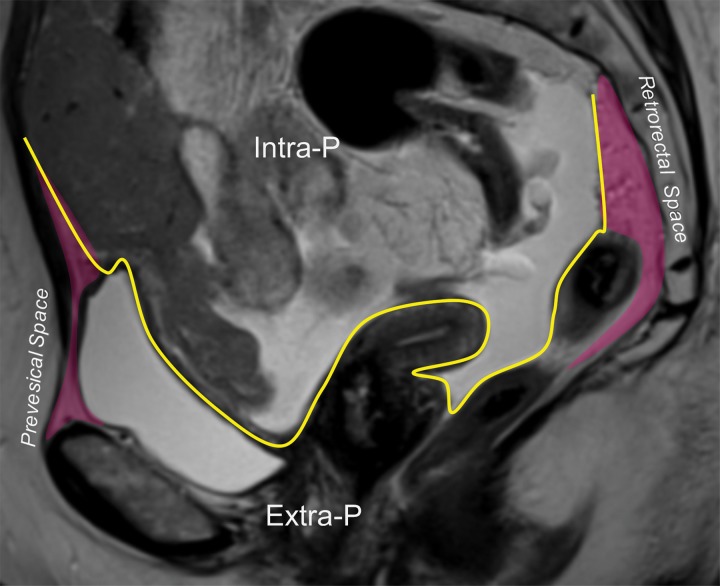
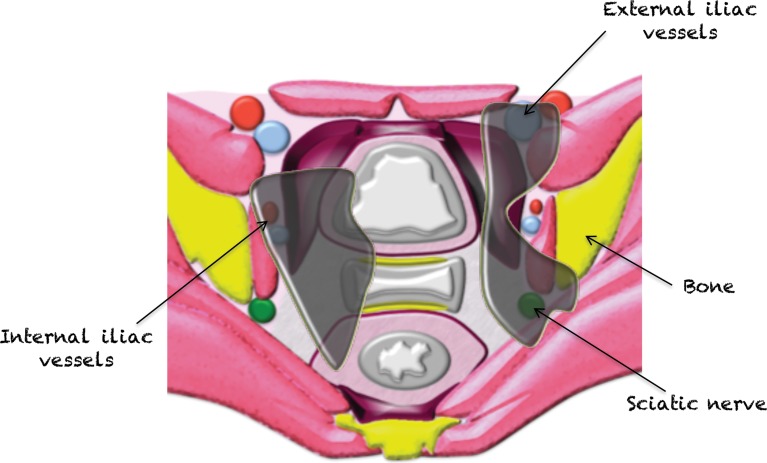
Pelvic masses can present a diagnostic challenge owing to the difficulty in assessing their origin and the overlap in imaging features. The majority of pelvic tumors arise from gastrointestinal or genitourinary organs, with less common sites of origin including the connective tissues, nerves, and lymphovascular structures. Lesion evaluation usually starts with clinical assessment followed by imaging, or the lesion may be an incidental finding at imaging performed for other clinical indications. Since accurate diagnosis is essential for optimal management, imaging is useful for suggesting the correct diagnosis or narrowing the differential possibilities and distinguishing tumors from their mimics. Some masses may require histologic confirmation of the diagnosis with biopsy and/or up-front surgical resection. In this case, imaging is essential for presurgical planning to assess mass size and location, evaluate the relationship to adjacent pelvic structures, and narrow differential possibilities. Pelvic US is often the first imaging modality performed in women with pelvic symptoms. While US is often useful to detect a pelvic mass, it has significant limitations in assessing masses located deep in the pelvis or near gas-filled organs. CT also has limited value in the pelvis owing to its inferior soft-tissue contrast. MRI is frequently the optimal imaging modality, as it offers both multiplanar capability and excellent soft-tissue contrast. This article highlights the normal anatomy of the pelvic spaces in the female pelvis and focuses on MRI features of common tumors and tumor mimics that arise in these spaces. It provides an interpretative algorithm for approaching an unknown pelvic lesion at MRI. It also discusses surgical management, emphasizing the value of MRI as a road map to surgery and highlighting anatomic locations where surgical resection may present a challenge. ©RSNA, 2019.
Figures




References
-
- Meyers M, Charnsangvej C, Oliphant M. Meyers’ dynamic radiology of the abdomen. New York, NY: Springer, 2011.
-
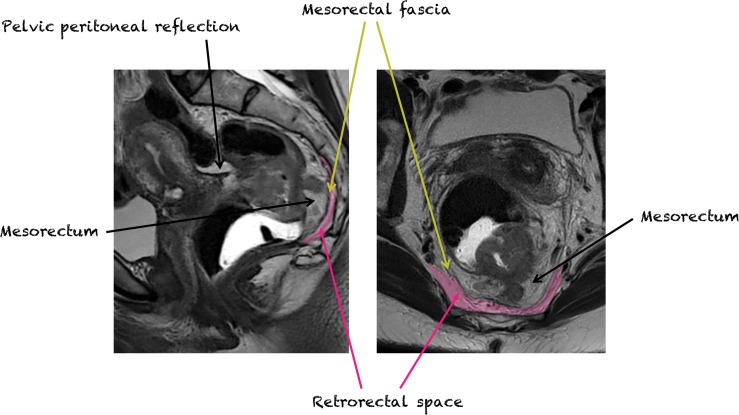
- Gollub MJ, Maas M, Weiser M, et al. . Recognition of the anterior peritoneal reflection at rectal MRI. AJR Am J Roentgenol 2013;200(1):97–101. - PubMed
-
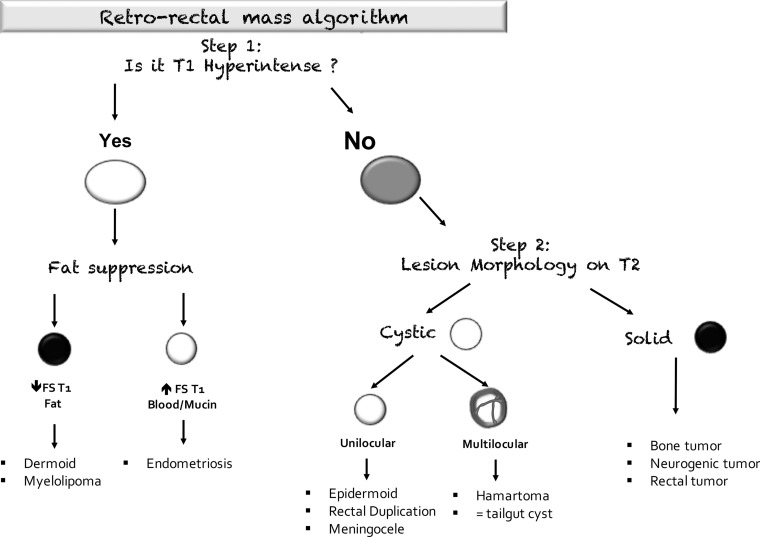
- Janvier A, Rousset P, Cazejust J, Bouché O, Soyer P, Hoeffel C. MR imaging of pelvic extraperitoneal masses: a diagnostic approach. Diagn Interv Imaging 2016;97(2):159–170. - PubMed
-
- Bazot M, Deligne L, Boudghène F, Buy JN, Lassau JP, Bigot JM. Correlation between computed tomography and gross anatomy of the suspensory ligament of the ovary. Surg Radiol Anat 1999;21(5):341–346. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
