

Prediction of Perioperative Mortality of Cadaveric Liver Transplant Recipients During Their Evaluations
- PMID: 31283673
- PMCID: PMC6756253
- DOI: 10.1097/TP.0000000000002810
Prediction of Perioperative Mortality of Cadaveric Liver Transplant Recipients During Their Evaluations
Abstract
Background: There are no instruments that can identify patients at an increased risk of poor outcomes after liver transplantation (LT) based only on their preoperative characteristics. The primary aim of this study was to develop such a scoring system. Secondary outcomes were to assess the discriminative performance of the predictive model for 90-day mortality, 1-year mortality, and 5-year patient survival.
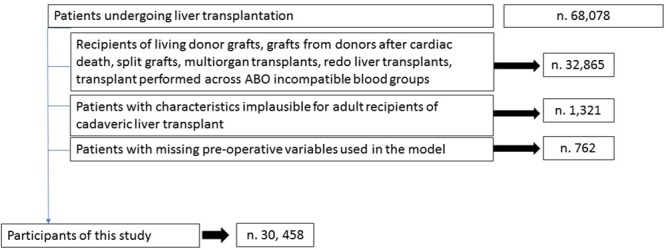
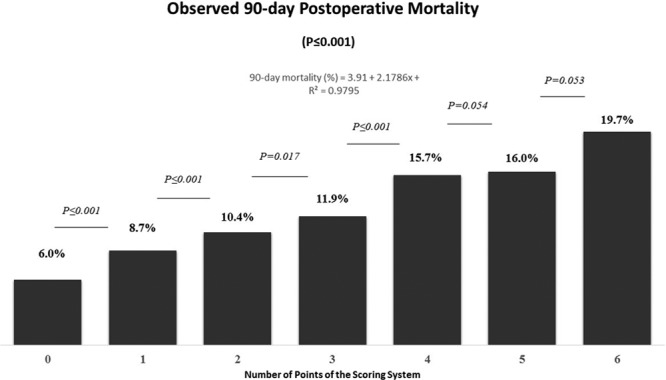
Methods: The study population was represented by 30 458 adults who underwent LT in the United States between January 2002 and June 2013. Machine learning techniques identified recipient age, Model for End-Stage Liver Disease score, body mass index, diabetes, and dialysis before LT as the strongest predictors for 90-day postoperative mortality. A weighted scoring system (minimum of 0 to a maximum of 6 points) was subsequently developed.
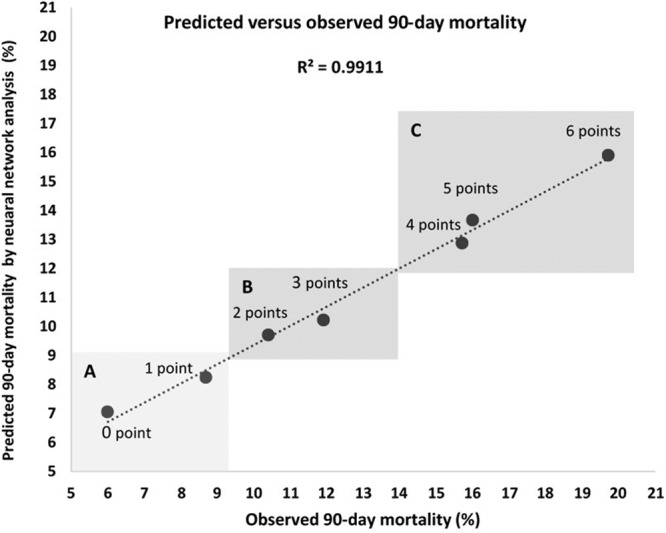
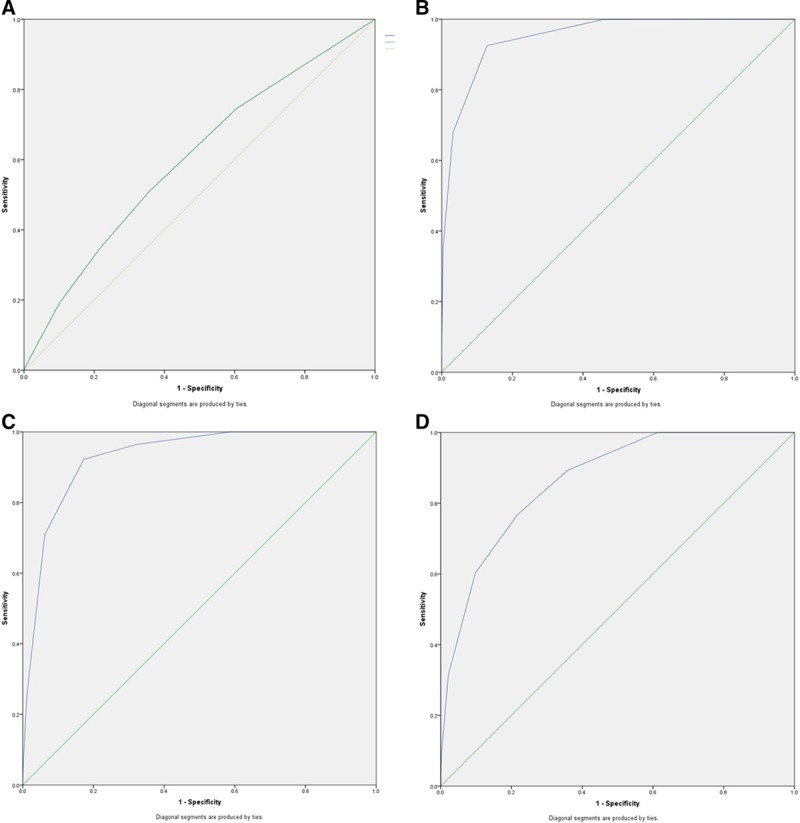
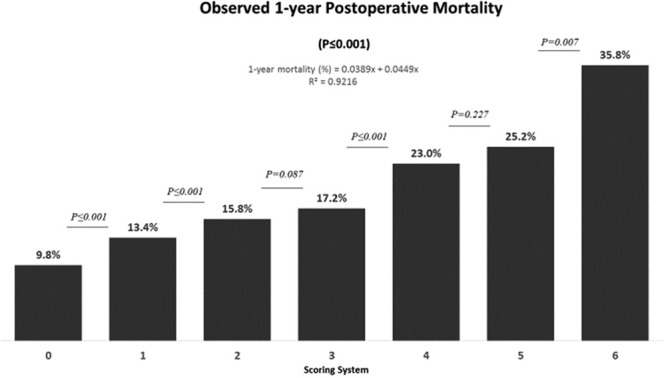
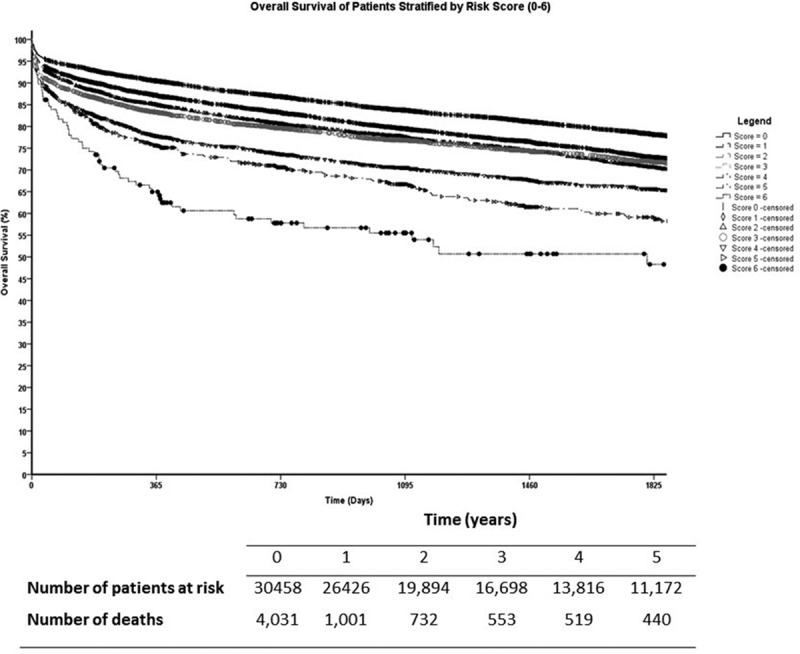
Results: Recipients with 0, 1, 2, 3, 4, 5, and 6 points had an observed 90-day mortality of 6.0%, 8.7%, 10.4%, 11.9%, 15.7%, 16.0%, and 19.7%, respectively (P ≤ 0.001). One-year mortality was 9.8%, 13.4%, 15.8%, 17.2%, 23.0%, 25.2%, and 35.8% (P ≤ 0.001) and five-year survival was 78%, 73%, 72%, 71%, 65%, 59%, and 48%, respectively (P = 0.001). The mean 90-day mortality for the cohort was 9%. The area under the curve of the model was 0.952 for the discrimination of patients with 90-day mortality risk ≥10%.
Conclusions: Short- and long-term outcomes of patients undergoing cadaveric LT can be predicted using a scoring system based on recipients' preoperative characteristics. This tool could assist clinicians and researchers in identifying patients at increased risks of postoperative death.
Figures
Comment in
-
Is it Still Tough to Make Predictions About the Future?Transplantation. 2019 Oct;103(10):1977. doi: 10.1097/TP.0000000000002839. Transplantation. 2019. PMID: 31233479 No abstract available.
-
Predicting Liver Transplant Patient Outcomes. Is a Validated Model Enough?Transplantation. 2020 Dec;104(12):2469-2470. doi: 10.1097/TP.0000000000003354. Transplantation. 2020. PMID: 32675740 No abstract available.
References
-
- Rana A, Ackah RL, Webb GJ, et al. No gains in long-term survival after liver transplantation over the past three decades. Ann Surg 201926920–27 - PubMed
-
- Dutkowski P, Oberkofler CE, Slankamenac K, et al. Are there better guidelines for allocation in liver transplantation? A novel score targeting justice and utility in the model for end-stage liver disease era. Ann Surg 2011254745–53Discussion 753 - PubMed
-
- Feng S, Goodrich NP, Bragg-Gresham JL, et al. Characteristics associated with liver graft failure: the concept of a donor risk index. Am J Transplant 20066783–790 - PubMed
-
- Halldorson JB, Bakthavatsalam R, Fix O, et al. D-MELD, a simple predictor of post liver transplant mortality for optimization of donor/recipient matching. Am J Transplant 20099318–326 - PubMed
-
- Rana A, Hardy MA, Halazun KJ, et al. Survival outcomes following liver transplantation (SOFT) score: a novel method to predict patient survival following liver transplantation. Am J Transplant 200882537–2546 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
