

Systematic Review and Meta-Analysis of Randomized, Controlled Trials on Preoperative Physical Exercise Interventions in Patients with Non-Small-Cell Lung Cancer
- PMID: 31284372
- PMCID: PMC6678369
- DOI: 10.3390/cancers11070944
Systematic Review and Meta-Analysis of Randomized, Controlled Trials on Preoperative Physical Exercise Interventions in Patients with Non-Small-Cell Lung Cancer
Abstract
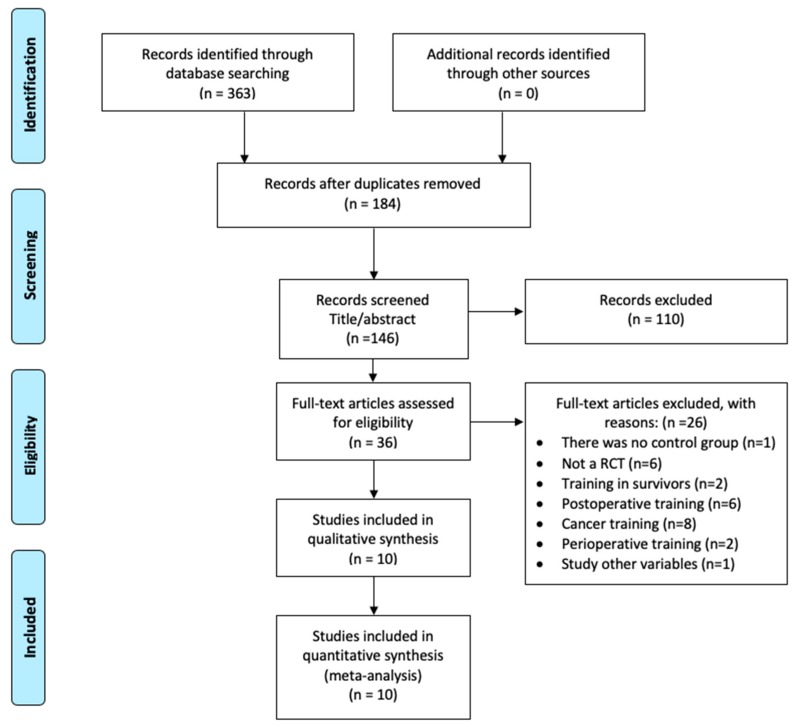
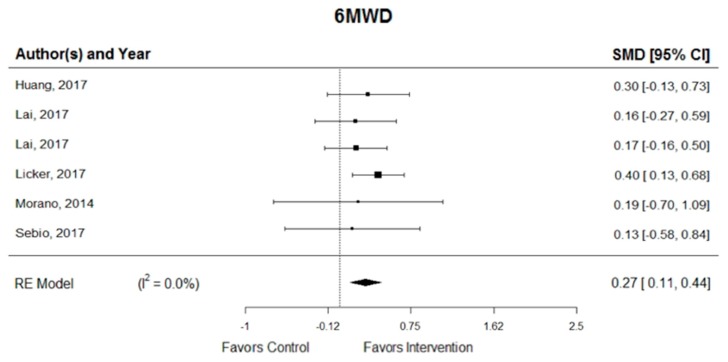
Preoperative physical exercise protocols prior to cancer surgery increased in popularity over recent years; however, the beneficial effect of such protocols is not well established, with conflicting results reported. We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) to assess the effects of different modalities or combinations of preoperative exercise interventions and/or prehabilitation multicomponent training in patients with non-small-cell lung cancer (NSCLC) after surgery on the outcomes related to functional capacity, mental wellness and medical care. We searched in OVID Embase, Pubmed, Cochrane Library, CINAHL, Scopus, and Web of Science. Characteristics of studies and program results and outcome data were extracted. Changes between the intervention and control groups, from baseline to follow-up (standardized mean difference (SMD) or relative risk (RR) with 95% confidence interval (CI) for each intervention was pooled using weighted random-effects models). A total of 676 participants from 10 RCTs were included in the final analysis (aerobic training + inspiratory muscle training, n = 5; aerobic training + strength training + inspiratory muscle training, n = 2; aerobic training + strength training, n = 1; multicomponent training, n = 1; aerobic training alone, n = 1). The results showed intervention-induced improvement in walking endurance (SMD = 0.27; 95% CI, 0.11 to 0.44; I2 = 0.0%), peak exercise capacity (SMD = 0.78; 95% CI, 0.35 to 1.21; I2 = 76.7%), dyspnoea (SMD = -0.30; 95% CI, -0.51 to -0.10; I2 = 0.0%), risk of hospitalization (SMD = -0.58; 95% CI, -0.97 to -0.20; I2 = 70.7%), and postoperative pulmonary complications (relative risk (RR) = 0.50; 95% CI, 0.39 to 0.66; I2 = 0.0%). For the functional capacity and medical care parameters, preoperative combined aerobic, resistance, and inspiratory muscle training was shown to be effective if comprising one to four weeks, performing 1-3 sessions per week, with moderate intensity (50% for endurance capacity). Further studies with larger samples and higher methodological quality are needed to clarify the potential benefits of preoperative exercise training for patients with NSCLC.
Keywords: cardiovascular; functional capacity; lung cancer; resistance training.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Sommer M., Trier K., Vibe-Petersen J., Missel M., Christensen M., Larsen K., Langer S., Hendriksen C., Clementsen P., Pedersen J., et al. Perioperative rehabilitation in operation for lung cancer (PROLUCA) rationale and design. BMC Cancer. 2014;14:404. doi: 10.1186/1471-2407-14-404. - DOI - PMC - PubMed
-
- National Institute for Health and Care Excellence Lung Cancer: Diagnosis and Management. [(accessed on 14 March 2019)]; Available online: https://www.nice.org.uk/guidance/cg121.
Publication types
LinkOut - more resources
Full Text Sources
Medical
