

Prognosis and Predictors of Mortality in Patients Suffering Myocardial Infarction With Non-Obstructive Coronary Arteries
- PMID: 31284804
- PMCID: PMC6662150
- DOI: 10.1161/JAHA.119.011990
Prognosis and Predictors of Mortality in Patients Suffering Myocardial Infarction With Non-Obstructive Coronary Arteries
Abstract
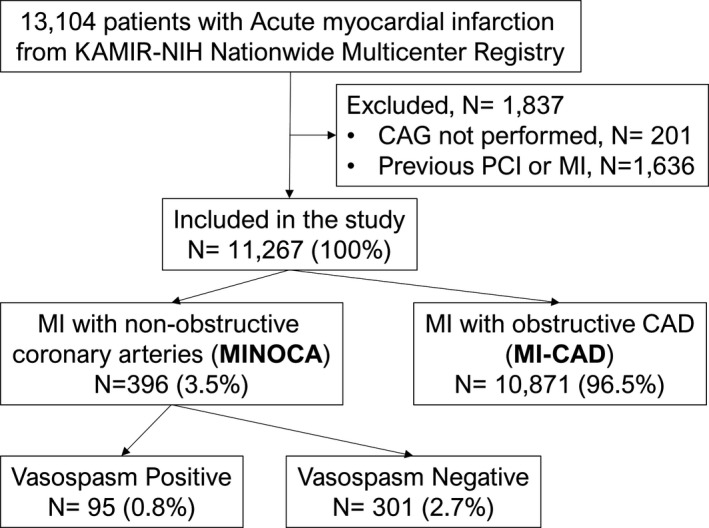
Background Myocardial infarction with nonobstructive coronary arteries ( MINOCA ) is a heterogeneous disease entity. Its prognosis and predictor of mortality remain unclear. This study aimed to compare the prognosis between MINOCA and myocardial infarction with obstructive coronary artery disease and identify factors related to all-cause death in MINOCA using a nation-wide, multicenter, and prospective registry. Methods and Results Among 13 104 consecutive patients enrolled, patients without previous history of significant coronary artery disease who underwent coronary angiography were selected. The primary outcome was 2-year all-cause death. Secondary outcomes were cardiac death, noncardiac death, reinfarction, and repeat revascularization. Patients with MINOCA (n=396) and myocardial infarction with obstructive coronary artery disease (n=10 871) showed similar incidence of all-cause death (9.1% versus 8.8%; hazard ratio [ HR ], 1.04; 95% CI, 0.74-1.45; P=0.83). Risks of cardiac death, noncardiac death, and reinfarction were not significantly different between the 2 groups ( HR , 0.82; 95% CI , 0.53-1.28; P=0.38; HR , 1.55; 95% CI , 0.93-2.56; P=0.09; HR , 1.23; 95% CI , 0.65-2.31; P=0.38, respectively). MINOCA patients had lower incidence of repeat revascularization (1.3% versus 7.2%; HR , 0.17; 95% CI , 0.07-0.41; P<0.001). Results were consistent after multivariable regression and propensity-score matching. In a multivariate model, several significant predictors of all-cause death of MINOCA were found, including the nonuse of renin-angiotensin system blockers ( HR , 2.63; 95% CI , 1.08-6.25; P=0.033) and statins ( HR , 2.17; 95% CI , 1.04-4.54; P=0.039). Conclusions Patients with MINOCA and those with myocardial infarction with obstructive coronary artery disease had comparable clinical outcomes. Use of renin-angiotensin system blockers and statins was associated with lower mortality in patients with MINOCA .
Keywords: coronary vasospasm; myocardial infarction; prognosis; renin angiotensin system; statin.
Figures

Comment in
-
Myocardial Infarction With Nonobstructive Coronary Arteries: A Call for Individualized Treatment.J Am Heart Assoc. 2019 Jul 16;8(14):e013361. doi: 10.1161/JAHA.119.013361. Epub 2019 Jul 9. J Am Heart Assoc. 2019. PMID: 31284819 Free PMC article.
References
-
- Agewall S, Beltrame JF, Reynolds HR, Niessner A, Rosano G, Caforio AL, De Caterina R, Zimarino M, Roffi M, Kjeldsen K, Atar D, Kaski JC, Sechtem U, Tornvall P. ESC working group position paper on myocardial infarction with non‐obstructive coronary arteries. Eur Heart J. 2017;38:143–153. - PubMed
-
- Roe MT, Harrington RA, Prosper DM, Pieper KS, Bhatt DL, Lincoff AM, Simoons ML, Akkerhuis M, Ohman EM, Kitt MM, Vahanian A, Ruzyllo W, Karsch K, Califf RM, Topol EJ. Clinical and therapeutic profile of patients presenting with acute coronary syndromes who do not have significant coronary artery disease. The Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrilin Therapy (PURSUIT) Trial Investigators. Circulation. 2000;102:1101–1106. - PubMed
-
- Diver DJ, Bier JD, Ferreira PE, Sharaf BL, McCabe C, Thompson B, Chaitman B, Williams DO, Braunwald E. Clinical and arteriographic characterization of patients with unstable angina without critical coronary arterial narrowing (from the TIMI‐IIIA Trial). Am J Cardiol. 1994;74:531–537. - PubMed
-
- Patel MR, Chen AY, Peterson ED, Newby LK, Pollack CV Jr, Brindis RG, Gibson CM, Kleiman NS, Saucedo JF, Bhatt DL, Gibler WB, Ohman EM, Harrington RA, Roe MT. Prevalence, predictors, and outcomes of patients with non‐ST‐segment elevation myocardial infarction and insignificant coronary artery disease: results from the Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines (CRUSADE) initiative. Am Heart J. 2006;152:641–647. - PubMed
-
- Dokainish H, Pillai M, Murphy SA, DiBattiste PM, Schweiger MJ, Lotfi A, Morrow DA, Cannon CP, Braunwald E, Lakkis N. Prognostic implications of elevated troponin in patients with suspected acute coronary syndrome but no critical epicardial coronary disease: a TACTICS‐TIMI‐18 substudy. J Am Coll Cardiol. 2005;45:19–24. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
