

Quadruple versus triple combination antiretroviral therapies for treatment naive people with HIV: systematic review and meta-analysis of randomised controlled trials
- PMID: 31285198
- PMCID: PMC6613201
- DOI: 10.1136/bmj.l4179
Quadruple versus triple combination antiretroviral therapies for treatment naive people with HIV: systematic review and meta-analysis of randomised controlled trials
Abstract
Objective: To evaluate the effects of four drug (quadruple) versus three drug (triple) combination antiretroviral therapies in treatment naive people with HIV, and explore the implications of existing trials for clinical practice and research.
Design: Systematic review and meta-analysis of randomised controlled trials.
Data sources: PubMed, EMBASE, CENTRAL, Web of Science, and the Cumulative Index to Nursing and Allied Health Literature from March 2001 to December 2016 (updated search in PubMed and EMBASE up to June 2018); and reference lists of eligible studies and related reviews.
Study selection: Randomised controlled trials comparing quadruple with triple combination antiretroviral therapies in treatment naive people with HIV and evaluating at least one effectiveness or safety outcome.
Review methods: Outcomes of interest included undetectable HIV-1 RNA, CD4 T cell count, virological failure, new AIDS defining events, death, and severe adverse effects. Random effects meta-analyses were conducted.
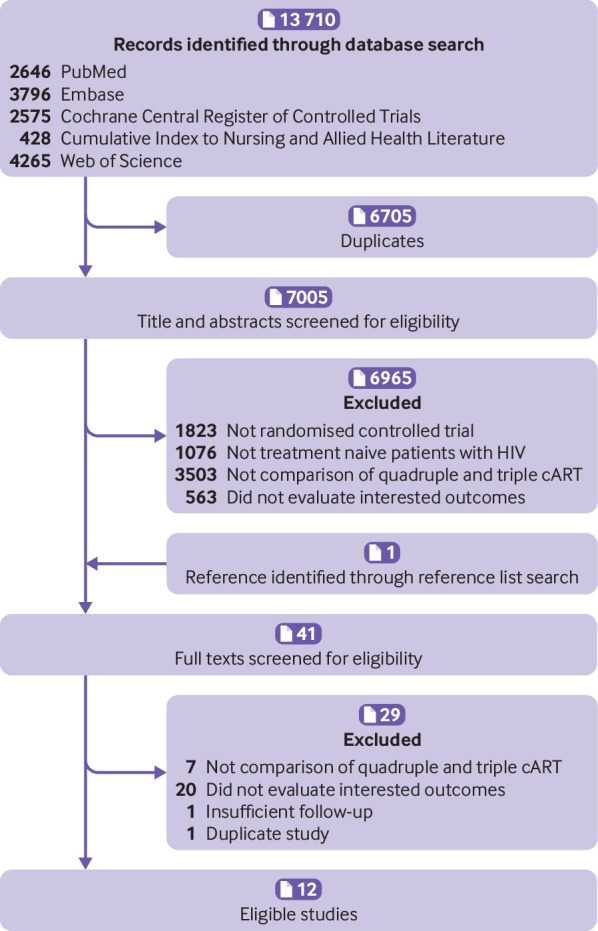
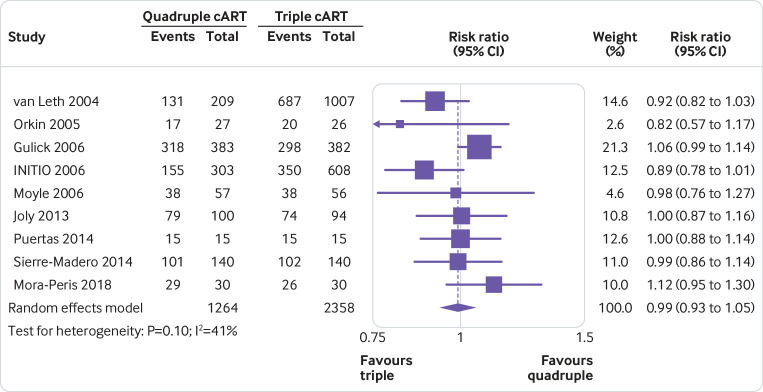
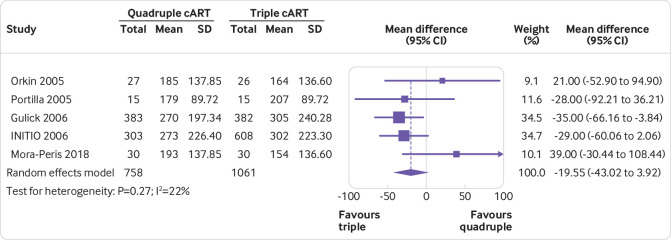
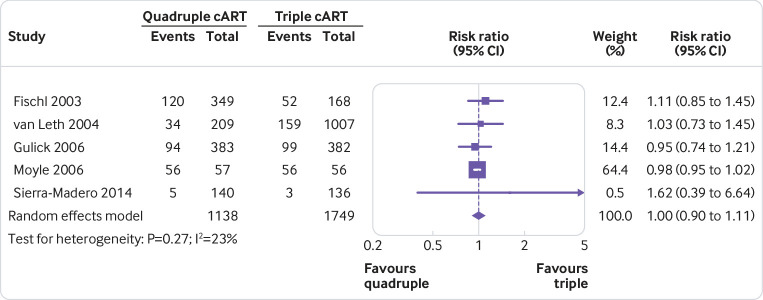
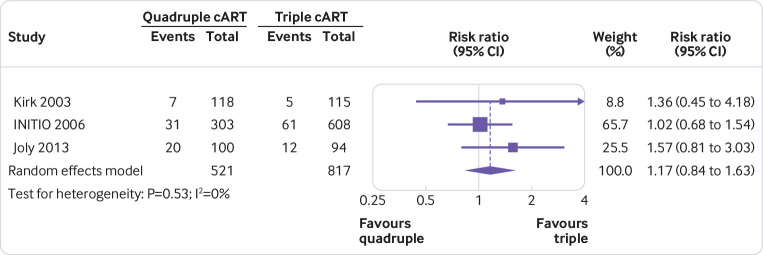
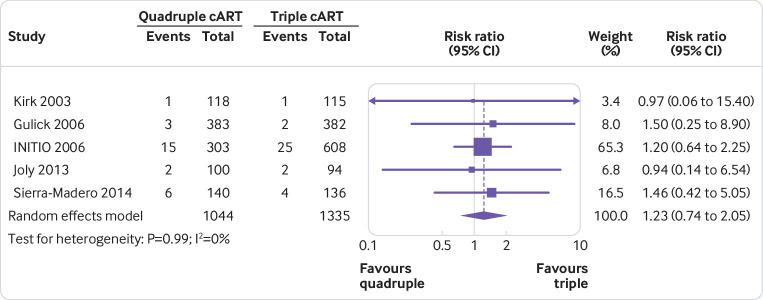
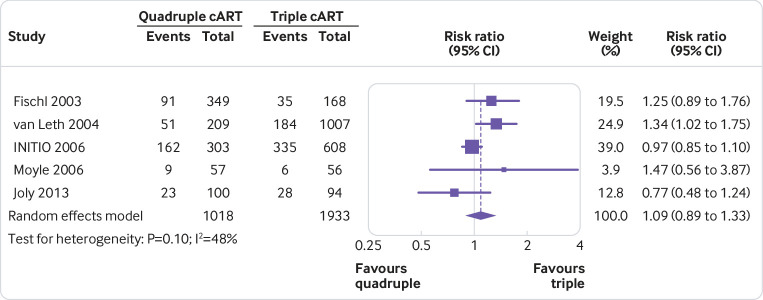
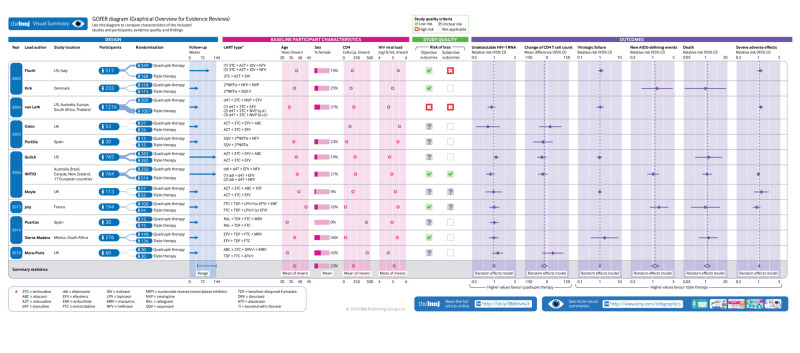
Results: Twelve trials (including 4251 people with HIV) were eligible. Quadruple and triple combination antiretroviral therapies had similar effects on all relevant effectiveness and safety outcomes, with no point estimates favouring quadruple therapy. With the triple therapy as the reference group, the risk ratio was 0.99 (95% confidence interval 0.93 to 1.05) for undetectable HIV-1 RNA, 1.00 (0.90 to 1.11) for virological failure, 1.17 (0.84 to 1.63) for new AIDS defining events, 1.23 (0.74 to 2.05) for death, and 1.09 (0.89 to 1.33) for severe adverse effects. The mean difference in CD4 T cell count increase between the two groups was -19.55 cells/μL (-43.02 to 3.92). In general, the results were similar, regardless of the specific regimens of combination antiretroviral therapies, and were robust in all subgroup and sensitivity analyses.
Conclusion: In this study, effects of quadruple combination antiretroviral therapy were not better than triple combination antiretroviral therapy in treatment naive people with HIV. This finding lends support to current guidelines recommending the triple regimen as first line treatment. Further trials on this topic should be conducted only when new research is justified by adequate systematic reviews of the existing evidence. However, this study cannot exclude the possibility that quadruple cART would be better than triple cART when new classes of antiretroviral drugs are made available.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure forms at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; MTM received grants from NIAAA US and NIHR HPRU UK; HZ received grants from the National Science Foundation of China Young Scientist Fund (81703278), National Science and Technology Major Project (China; 2018ZX10721102), Sanming Project of Medicine (Shenzhen; SZSM201811071), and Australian National Health and Medical Research Council Early Career Fellowship (APP1092621); the other authors had no financial relationships with any organisations that might have an interest in the submitted work in the precious three years; no other relationship or activities that could appear to have influenced the submitted work.
Figures
References
-
- World Health Organization. Summary of the global HIV epidemic (2017). https://www.who.int/hiv/data/en/ Accessed 05 Dec 2018.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials