

Paramedic-initiated helivac to tertiary hospital for primary percutaneous coronary intervention: a strategy for improving treatment delivery times
- PMID: 31285874
- PMCID: PMC6588767
- DOI: 10.21037/jtd.2019.05.45
Paramedic-initiated helivac to tertiary hospital for primary percutaneous coronary intervention: a strategy for improving treatment delivery times
Abstract
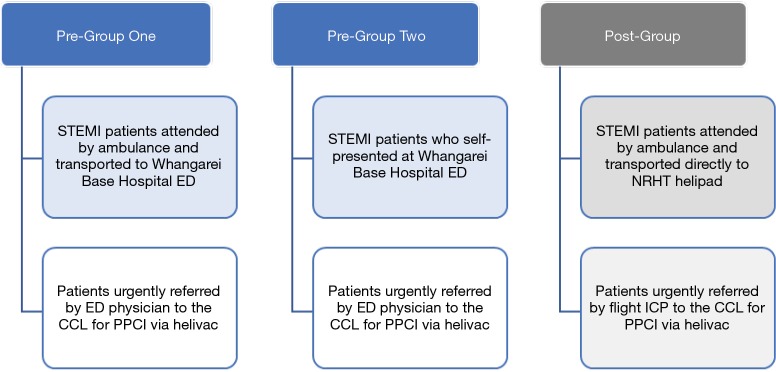
Background: In regions of New Zealand without coronary catheterisation laboratory (CCL) facilities, patients presenting with ST-elevation myocardial infarction (STEMI) are often subjected to prolonged delays before receiving primary percutaneous coronary intervention (PPCI) if it is the chosen reperfusion strategy. Therefore, we aimed to trial a new process of paramedic-initiated helivac of STEMI patients from the field directly to the CCL.
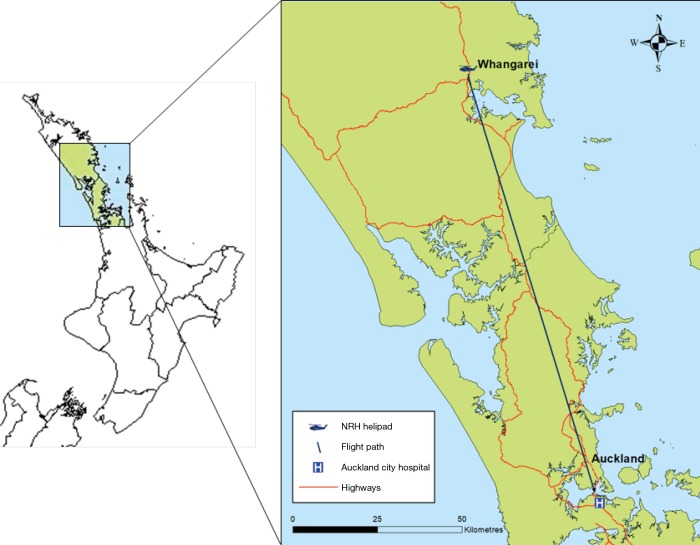
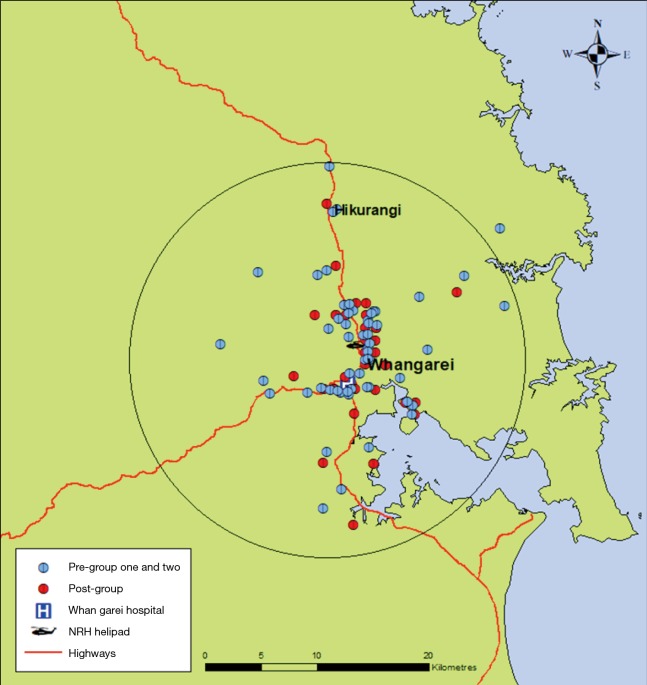
Methods: Utilising a prospective observational approach, over a 48-month period, paramedics identified patients with a clinical presentation and electrocardiogram features consistent with STEMI and transported them directly to the regional air ambulance base for helivac to the CCL (flight time 30-35 minutes). These patients were compared to two historic STEMI cohorts either transported by paramedics to the region's local hospital or self-presenting, prior to helivac. The primary outcome measures were: first medical contact-to-balloon (FMCTB) time and accuracy of paramedic diagnosis. Secondary outcome measures were mortality at 30 days and six months, and hospital length of stay (LOS).
Results: A total of 92 patients underwent helivac for PPCI (mean age of 64 years, SD ±10.3). Median FMCTB time was 155 minutes (IQR 27) for the historic cohorts (n=57), versus 102 minutes (IQR 16) for the experimental cohort (n=35, P<0.001). Paramedic diagnosis showed a sensitivity of 97% (95% CI: 85 to 99) and a specificity of 100% (95% CI: 84 to 100) with no inappropriate CCL activations. No significant difference was observed between groups in terms of 30 day and 6-month mortality. Hospital LOS was significantly shorter among the experimental cohort (P=0.01).
Conclusions: Paramedic-initiated helivac of STEMI patients from the field directly to the CCL for PPCI is safe and feasible and can significantly improve time-to-treatment to within benchmark timeframes, resulting in reduced hospital LOS.
Keywords: ST-elevation myocardial infarction (STEMI); air ambulances; ambulances; emergency medical services (EMS); percutaneous coronary intervention (PCI).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Paramedic-Delivered Fibrinolysis in the Treatment of ST-Elevation Myocardial Infarction: Comparison of a Physician-Authorized versus Autonomous Paramedic Approach.Prehosp Emerg Care. 2020 Sep-Oct;24(5):617-624. doi: 10.1080/10903127.2019.1683661. Epub 2019 Nov 13. Prehosp Emerg Care. 2020. PMID: 31718381
-
Paramedic contact to balloon in less than 90 minutes: a successful strategy for st-segment elevation myocardial infarction bypass to primary percutaneous coronary intervention in a canadian emergency medical system.Prehosp Emerg Care. 2011 Oct-Dec;15(4):490-8. doi: 10.3109/10903127.2011.598613. Epub 2011 Aug 10. Prehosp Emerg Care. 2011. PMID: 21830918
-
Weekly Checks Improve Real-Time Prehospital ECG Transmission in Suspected STEMI.Prehosp Disaster Med. 2018 Jun;33(3):245-249. doi: 10.1017/S1049023X18000341. Epub 2018 Apr 30. Prehosp Disaster Med. 2018. PMID: 29708085
-
Primary percutaneous coronary intervention for patients presenting with ST-elevation myocardial infarction: process improvements in rural prehospital care delivered by emergency medical services.Prog Cardiovasc Dis. 2010 Nov-Dec;53(3):210-8. doi: 10.1016/j.pcad.2010.09.003. Prog Cardiovasc Dis. 2010. PMID: 21130918
-
Comparison of early mortality of paramedic-diagnosed ST-segment elevation myocardial infarction with immediate transport to a designated primary percutaneous coronary intervention center to that of similar patients transported to the nearest hospital.Am J Cardiol. 2006 Nov 15;98(10):1329-33. doi: 10.1016/j.amjcard.2006.06.019. Epub 2006 Sep 28. Am J Cardiol. 2006. PMID: 17134623
References
-
- Ibanez B, James S, Agewall S, Antunes MJ, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2018;39:119-77. 10.1093/eurheartj/ehx393 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous