

Regionalization of thoracic surgery improves short-term cancer esophagectomy outcomes
- PMID: 31285879
- PMCID: PMC6588736
- DOI: 10.21037/jtd.2019.05.30
Regionalization of thoracic surgery improves short-term cancer esophagectomy outcomes
Abstract
Background: Some studies have found that outcomes from cancer esophagectomy are better at higher-volume centers than at lower-volume centers. Reports on outcomes following systematic centralization have largely demonstrated subsequent improvements, but these originate in nationalized healthcare systems that are not very comparable to the heterogeneous private-payer systems that predominate in the United States. We examined how regionalization of thoracic surgery to Centers of Excellence (CoE) within our American integrated healthcare system changed overall care for our patients, and whether it changed outcomes.
Methods: We conducted a retrospective chart review of 461 consecutive patients undergoing cancer esophagectomy between 2009-2016, spanning the 2014 shift to regionalization. High-volume was defined as ≥5 esophagectomies per year. We compared characteristics of the surgeon, hospital, and operation pre- and post-regionalization using Chi-square or Fisher's exact test for categorical variables and Kruskal-Wallis test for age. We evaluated their associations with patient outcomes with hierarchical linear and logistic mixed models, which adjusted for clustering within surgeon and facility levels and relevant covariates.
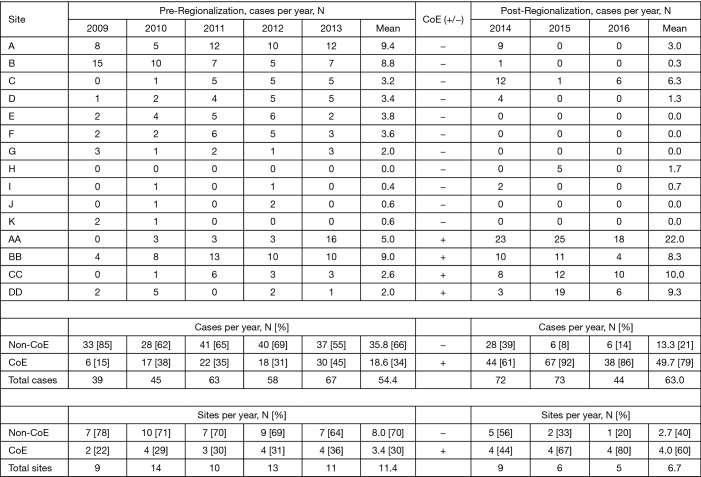
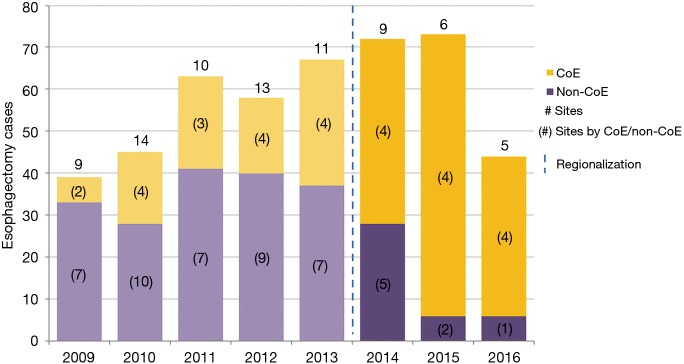
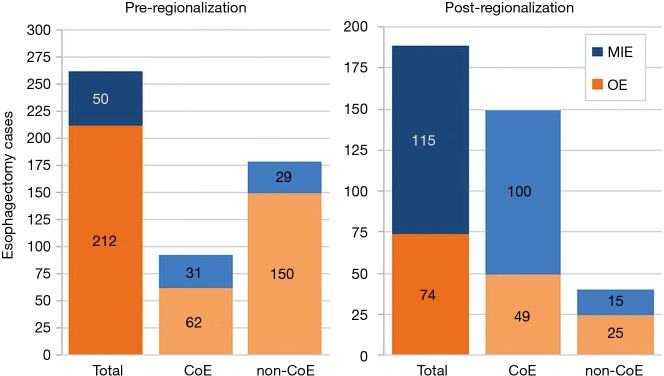
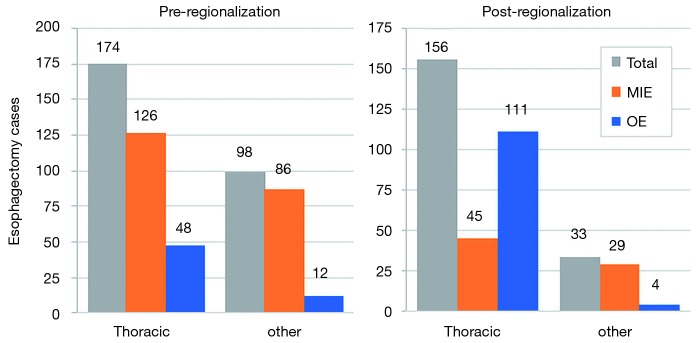
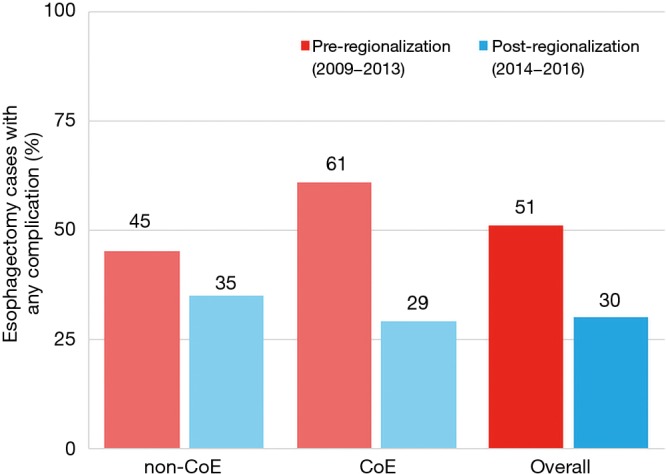
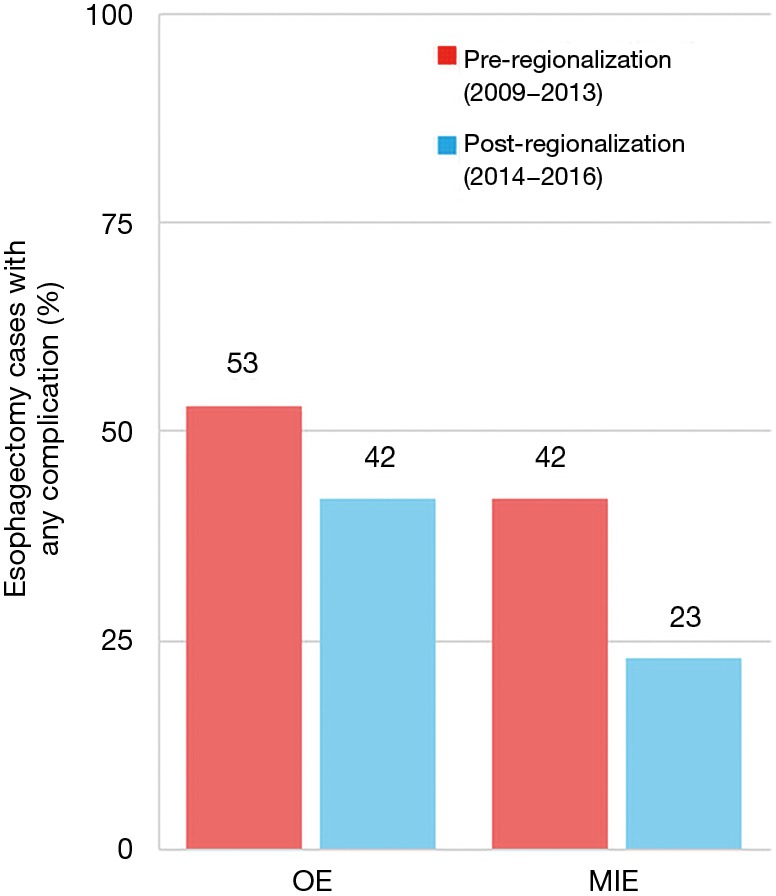
Results: While there was no difference in their baseline demographics, patients undergoing esophagectomy post-regionalization were much more likely to have their surgery performed at a designated Center of Excellence (78.8% of cases versus 34.2%, P<0.001), at a high-volume hospital (92.1% from 75.7%, P<0.001), by a high-volume surgeon (78.8% from 58.8%, P<0.001), by a board-certified thoracic surgeon (82.5% from 64.0%, P<0.001), and by minimally-invasive, versus open, approach (60.8% from 22.1%, P<0.001). Post-regionalization patients were in higher American Society of Anesthesiologists classes (P=0.03) and trended toward higher-stage disease (P=0.14), indicative of the inclusion of higher-complexity patients. Despite that, regionalization was associated with improved short-term outcomes, most notably: average minimally-invasive esophagectomy (MIE) operative time decreased by 2 hours (-135.9 minutes, 95% CI: -172.2, -99.7 minutes); length of stay (LOS) decreased by 2.3 days (95% CI: -3.4, -1.2 days); and 30-day complication rate decreased significantly, from 50.7% to 30.2% (OR 0.45, 95% CI: 0.25, 0.79). Regionalization was the only variable significantly and independently associated with all three outcomes in our adjusted multivariable models. Mortality, both at 30 and 90 days, decreased modestly but was low pre-regionalization, and the difference did not reach significance.
Conclusions: Regionalization of thoracic surgery in our hospital system resulted in esophagectomies being performed by more experienced surgeons at higher-volume centers, with a concomitant improvement in short-term outcomes. Patients undergoing esophagectomy, particularly MIE, post-regionalization benefited significantly from decreased LOS and perioperative complication rate. Our results suggest that, in a large integrated healthcare system, regionalization significantly improves overall outcomes for patients undergoing cancer esophagectomy.
Keywords: Esophagectomy; esophageal neoplasms; low-volume & high-volume hospitals; thoracic surgery.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Effect of Thoracic Surgery Regionalization on 1- and 3-Year Survival after Cancer Esophagectomy.Ann Surg. 2023 Feb 1;277(2):e305-e312. doi: 10.1097/SLA.0000000000005076. Epub 2023 Jan 10. Ann Surg. 2023. PMID: 34261883
-
Effect of thoracic surgery regionalization on long-term survival after lung cancer resection.J Thorac Cardiovasc Surg. 2022 Mar;163(3):769-777. doi: 10.1016/j.jtcvs.2021.03.050. Epub 2021 Mar 20. J Thorac Cardiovasc Surg. 2022. PMID: 33934900
-
Long-Term Impact of Regionalization of Thoracic Oncology Surgery.Ann Thorac Surg. 2025 Feb;119(2):460-469. doi: 10.1016/j.athoracsur.2024.10.002. Epub 2024 Oct 21. Ann Thorac Surg. 2025. PMID: 39442904
-
Refining the thoracic surgical oncology regionalization standards for esophageal surgery in Ontario, Canada: Moving from good to better.J Thorac Cardiovasc Surg. 2023 Dec;166(6):1502-1509. doi: 10.1016/j.jtcvs.2023.03.002. Epub 2023 Mar 10. J Thorac Cardiovasc Surg. 2023. PMID: 37005118 Review.
-
Regionalization of esophagectomy: where are we now?J Thorac Dis. 2019 Aug;11(Suppl 12):S1633-S1642. doi: 10.21037/jtd.2019.07.88. J Thorac Dis. 2019. PMID: 31489231 Free PMC article. Review.
Cited by
-
Regionalization for thoracic surgery: Economic implications of regionalization in the United States.J Thorac Cardiovasc Surg. 2021 May;161(5):1705-1709. doi: 10.1016/j.jtcvs.2020.10.132. Epub 2020 Nov 19. J Thorac Cardiovasc Surg. 2021. PMID: 33323196 Free PMC article.
-
Improving outcomes in malignant pleural mesothelioma in an integrated health care system.J Thorac Dis. 2022 Sep;14(9):3352-3363. doi: 10.21037/jtd-22-427. J Thorac Dis. 2022. PMID: 36245635 Free PMC article.
-
Evaluation of oesophageal and gastric resection outcomes in a small-volume unit.Ann Med Surg (Lond). 2021 Jun 11;67:102499. doi: 10.1016/j.amsu.2021.102499. eCollection 2021 Jul. Ann Med Surg (Lond). 2021. PMID: 34188911 Free PMC article.
-
Essential Updates 2018/2019: Essential Updates for esophageal cancer surgery.Ann Gastroenterol Surg. 2020 Feb 18;4(3):190-194. doi: 10.1002/ags3.12319. eCollection 2020 May. Ann Gastroenterol Surg. 2020. PMID: 32490332 Free PMC article. Review.
-
Recognizing the Role for Conversion Therapy in Metastatic Esophageal Squamous Cell Cancer (ESCC): A Call for Future Study.Ann Surg Oncol. 2025 Jan;32(1):24-26. doi: 10.1245/s10434-024-16335-0. Epub 2024 Oct 7. Ann Surg Oncol. 2025. PMID: 39375259 No abstract available.
References
-
- Cancer Stat Facts: Esophageal Cancer [Internet]. National Cancer Institute: Surveillance, Epidemiology, and End Results Program [cited 2017 Oct 15]. Available online: https://seer.cancer.gov/statfacts/html/esoph.html