

Transcatheter versus surgical aortic valve replacement in low and intermediate risk patients with severe aortic stenosis: systematic review and meta-analysis of randomized controlled trials and propensity score matching observational studies
- PMID: 31285888
- PMCID: PMC6588740
- DOI: 10.21037/jtd.2019.04.97
Transcatheter versus surgical aortic valve replacement in low and intermediate risk patients with severe aortic stenosis: systematic review and meta-analysis of randomized controlled trials and propensity score matching observational studies
Abstract
Background: To compare the outcome of transcatheter aortic valve replacement (TAVR) with surgical aortic valve replacement (SAVR) in low and intermediate risk patients with severe aortic stenosis (AS). Randomized controlled trials (RCT) and propensity score matching (PSM) studies compare TAVR with SAVR in patients at low and intermediate surgical risk.
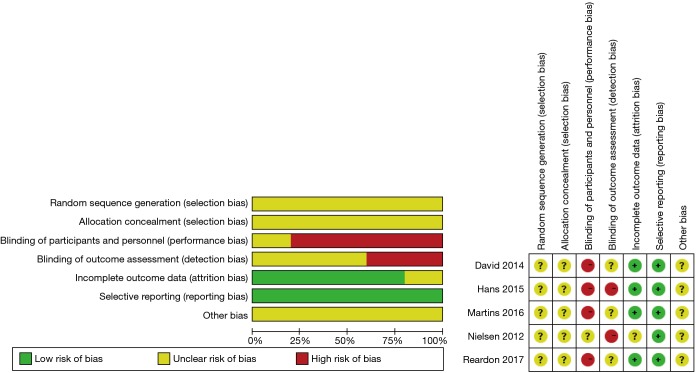
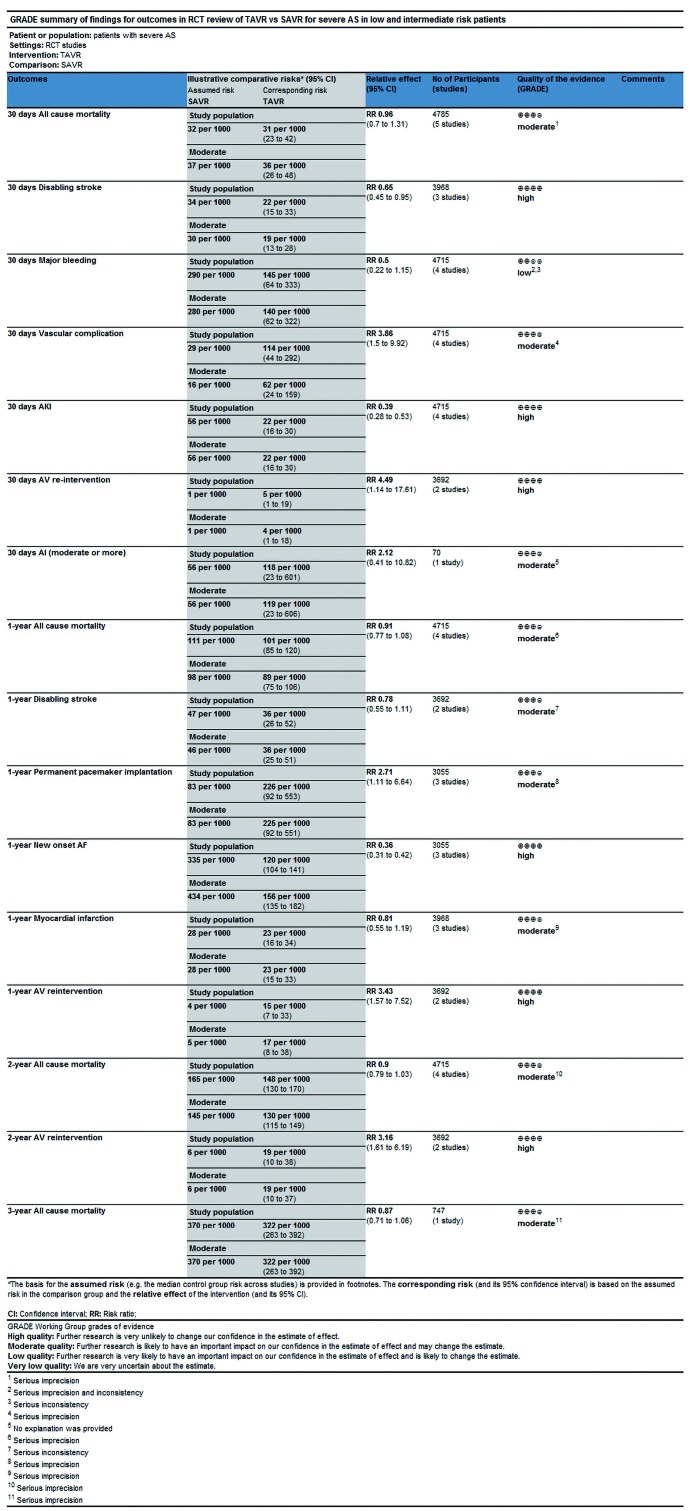
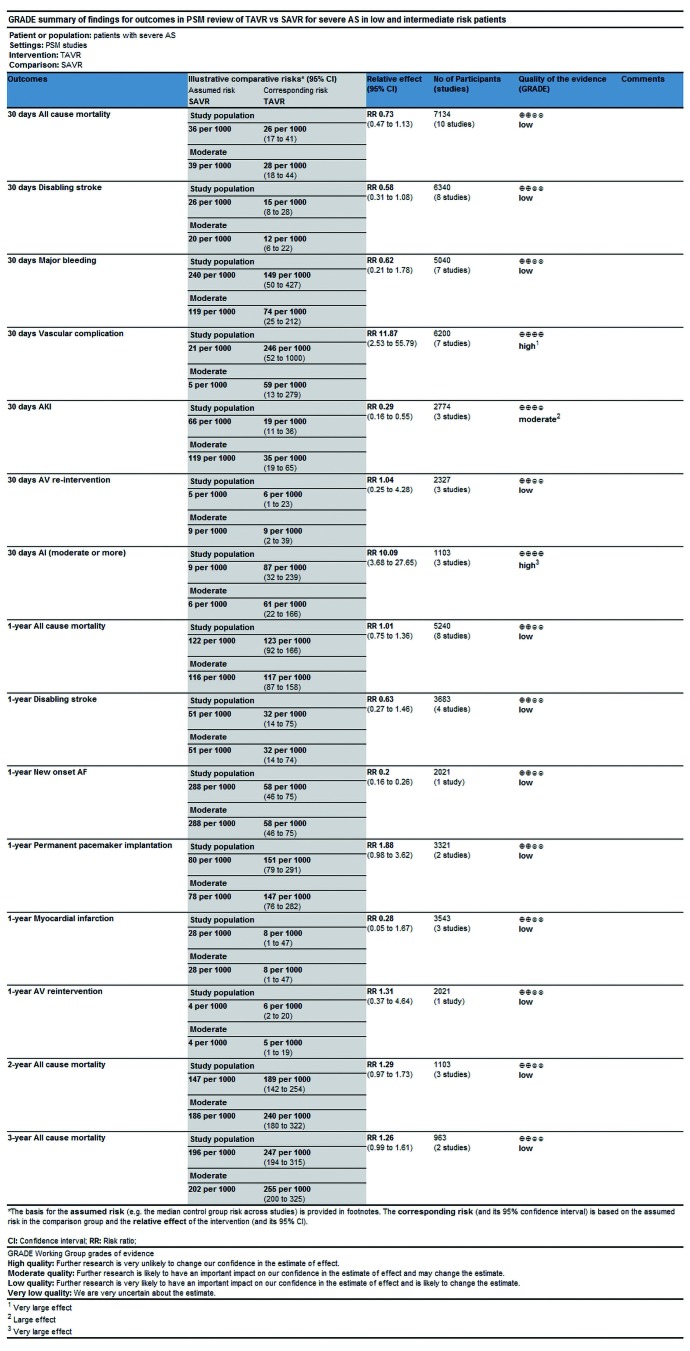
Methods: Two authors searched relevant literature independently, then extracted data from the included studies, and assessed risk of bias and quality of study separately according to different study designs, besides that, the extracted data was analyzed via utilization of GRADE system to evaluate the quality of evidence separately.
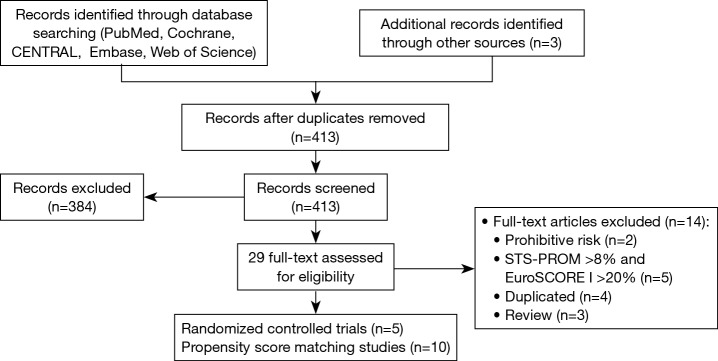
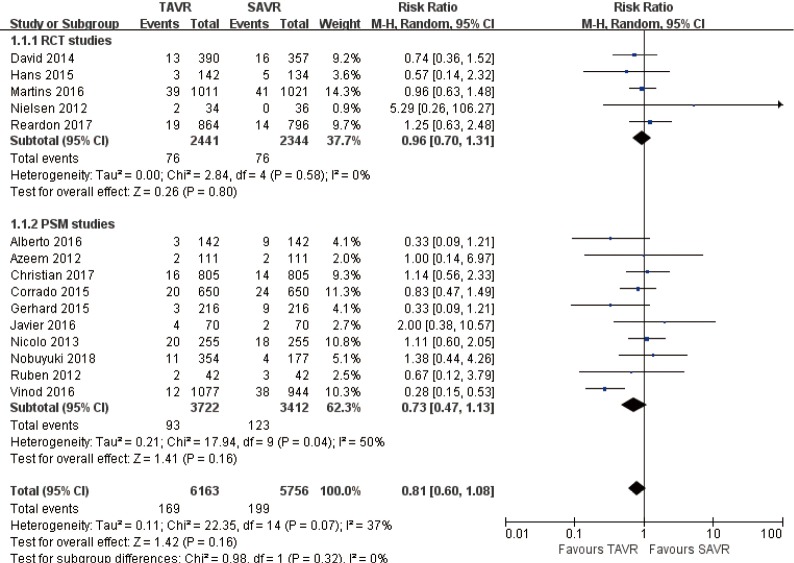
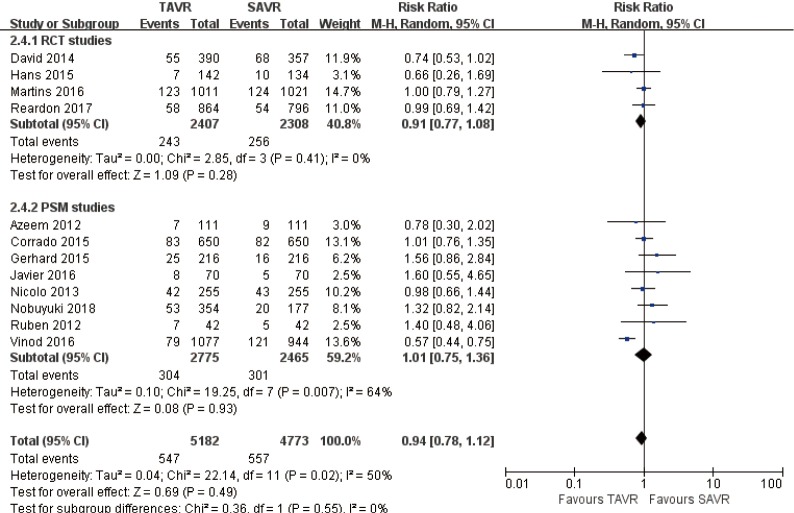
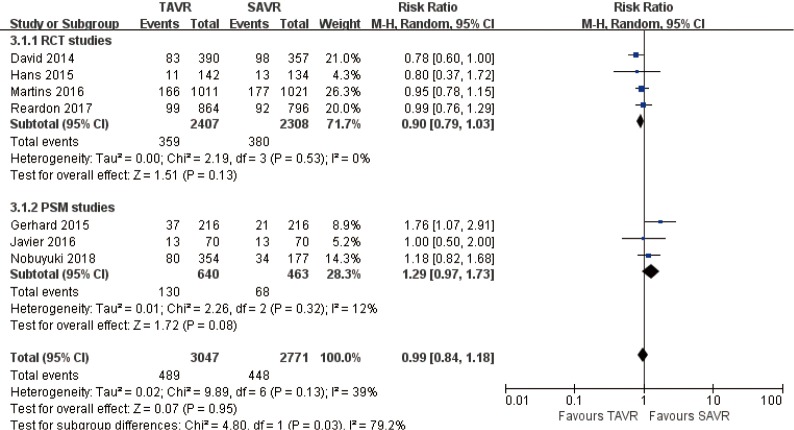
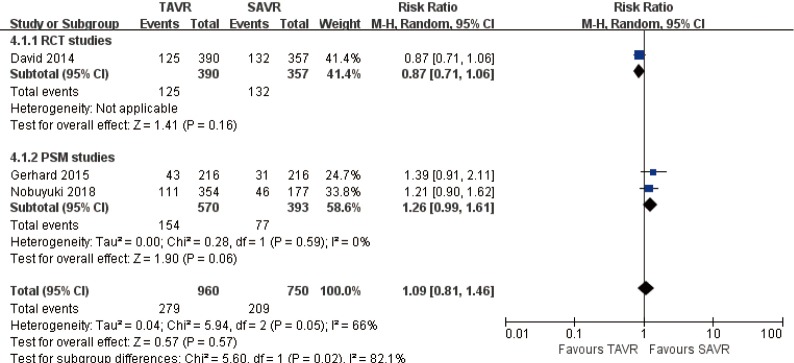
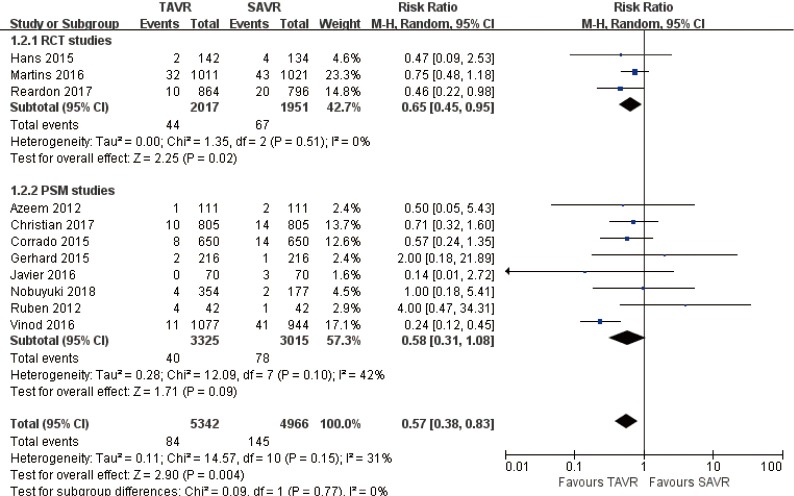
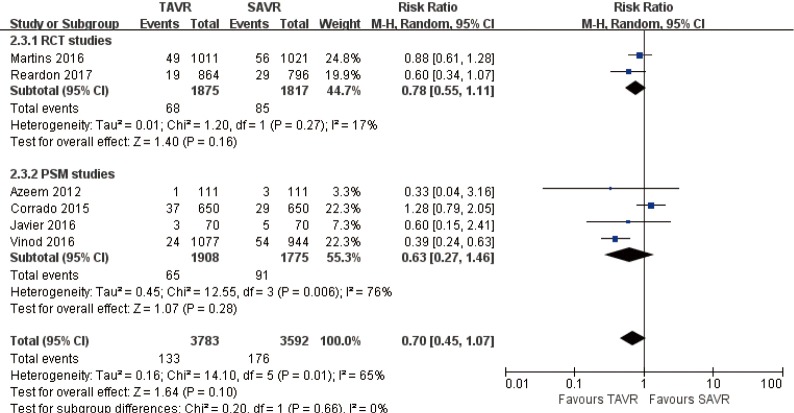
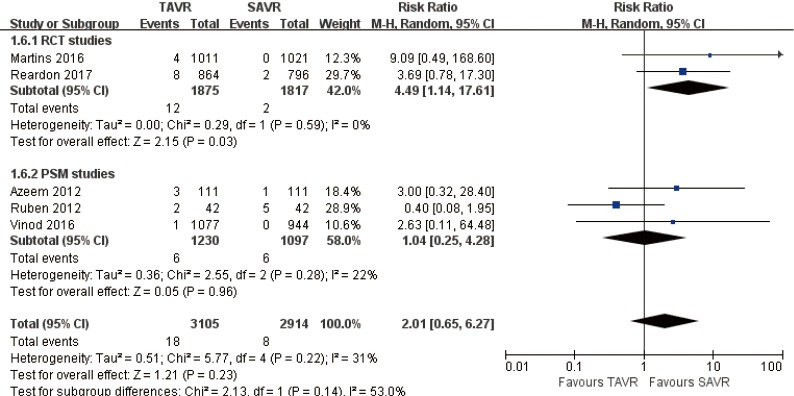
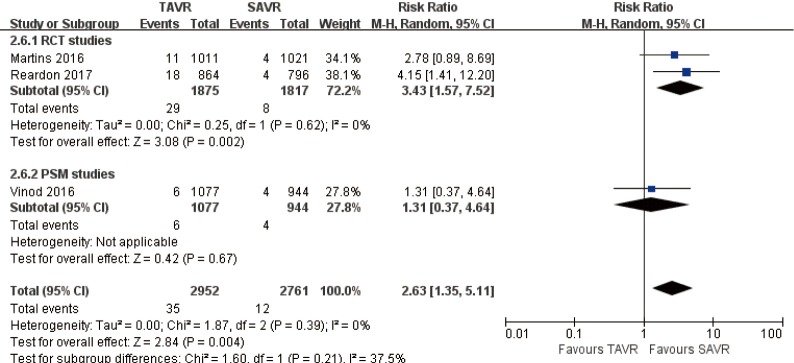
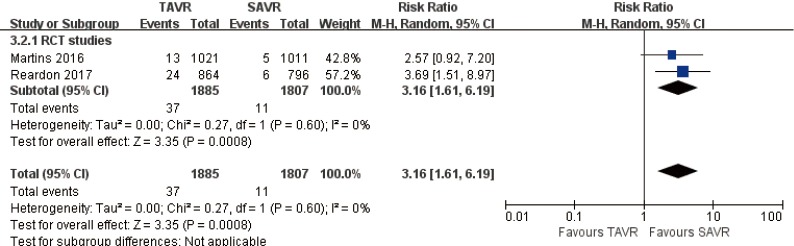
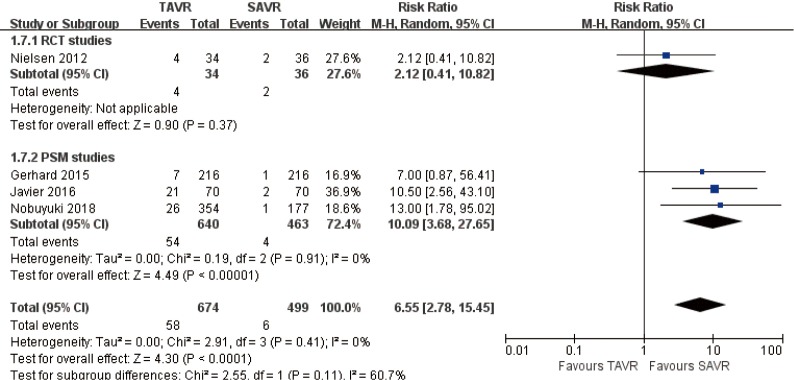
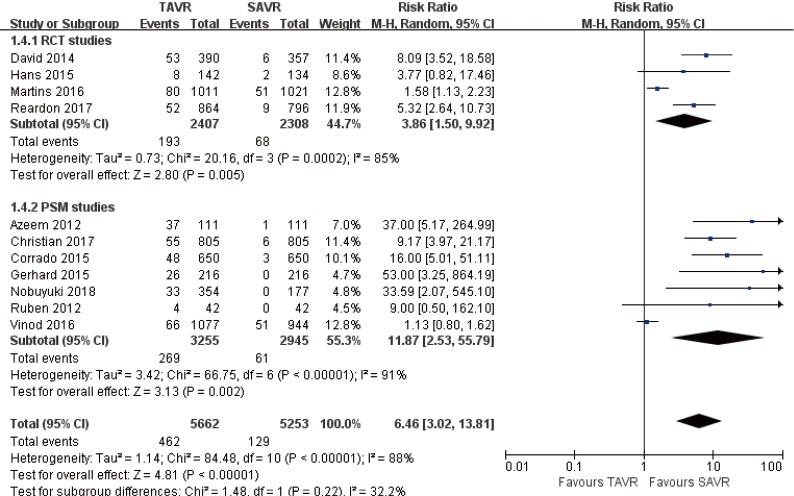
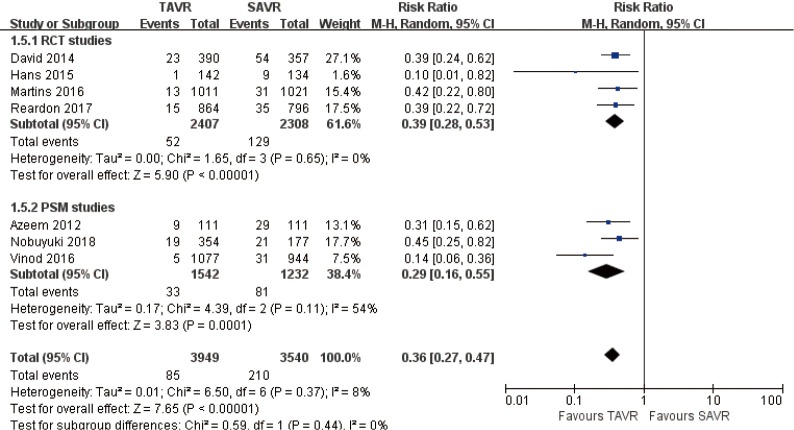
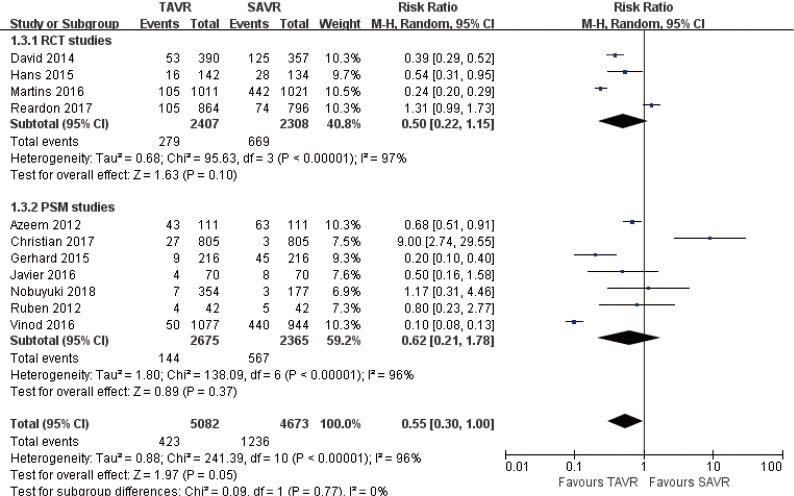
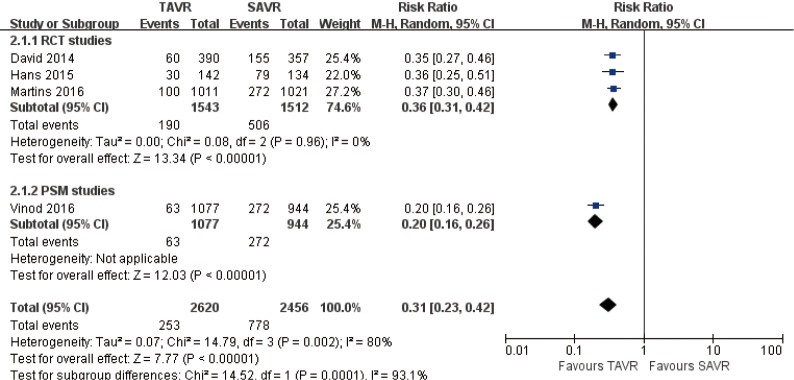
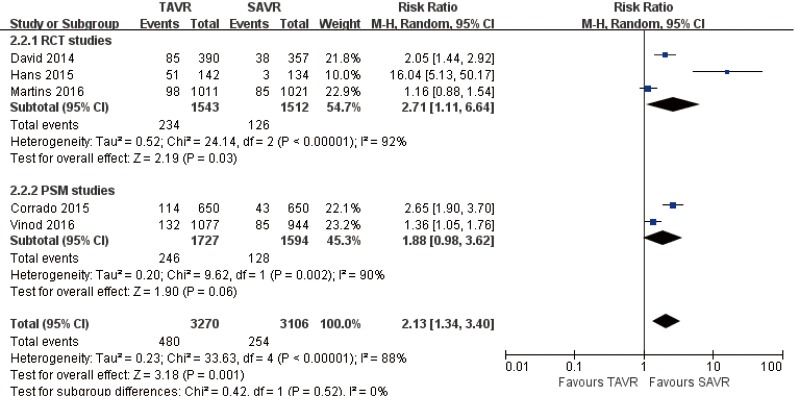
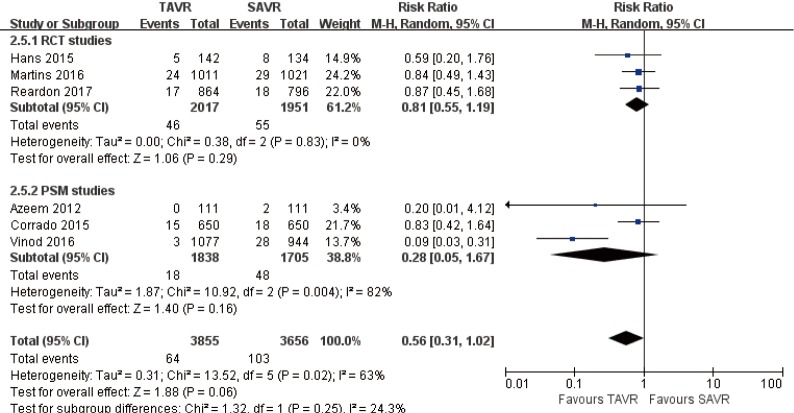
Results: Overall 15 studies (5 RCTs, 10 PSM studies) with total 12,057 patients were selected. Mortality and disabling stroke during follow-up period were comparable between TAVR and SAVR (RR 1.09, 95% CI: 0.81 to 1.46; RR 0.7, 95% CI: 0.45 to 1.07, respectively), TAVR revealed to be superior to SAVR regarding acute kidney injury (AKI), and onset of new atrial fibrillation (AF) (RCT: high certainty; AKI in PSM: moderate certainty, AF in PSM: low certainty). These results of RCT and PSM studies are consistent. In RCT review, SAVR was better in the following aspects: aortic valve (AV) re-intervention (high certainty), vascular complications, pacemaker implantation (moderate certainty), but comparable in the following aspects: myocardial infarction (MI), aortic insufficient (AI) (moderate certainty), major bleeding (low certainty). In PSM review, SAVR revealed a better result in AI and vascular complications (high certainty), but in the aspects of AV re-intervention, pacemaker implantation, major bleeding and MI (low certainty), it was comparable.
Conclusions: TAVR is comparable to SAVR in terms of mortality and disabling stroke in severe AS patients at low and intermediate risk, but higher proportion of AV re-intervention observed in TAVR. Those results should encourage caution when extending the indications of TAVR into low risk patients, especially for young low risk patients.
Systematic review registration: PROSPERO CRD 42018112626.
Keywords: Transcatheter aortic valve replacement (TAVR); low and intermediate risk; meta-analysis; severe aortic stenosis; surgical aortic valve replacement (SAVR).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Transcatheter aortic valve implantation versus surgical aortic valve replacement for severe aortic stenosis in people with low surgical risk.Cochrane Database Syst Rev. 2019 Dec 20;12(12):CD013319. doi: 10.1002/14651858.CD013319.pub2. Cochrane Database Syst Rev. 2019. PMID: 31860123 Free PMC article.
-
[Comparison on the prognosis of severe aortic stenosis patients treated with transcatheter aortic valve replacement versus surgical aortic valve replacement: a systematic review and meta-analysis].Zhonghua Xin Xue Guan Bing Za Zhi. 2022 Sep 24;50(9):913-919. doi: 10.3760/cma.j.cn112148-20220211-00100. Zhonghua Xin Xue Guan Bing Za Zhi. 2022. PMID: 36096710 Chinese.
-
Transcatheter versus surgical aortic valve replacement in patients at low surgical risk: A meta-analysis of randomized trials and propensity score matched observational studies.Catheter Cardiovasc Interv. 2018 Aug 1;92(2):408-416. doi: 10.1002/ccd.27518. Epub 2018 Feb 1. Catheter Cardiovasc Interv. 2018. PMID: 29388308
-
Transcatheter Versus Surgical Aortic Valve Replacement in Low-Risk Patients.J Am Coll Cardiol. 2019 Sep 24;74(12):1532-1540. doi: 10.1016/j.jacc.2019.06.076. J Am Coll Cardiol. 2019. PMID: 31537261
-
Transcatheter aortic valve implantation versus surgical aortic valve replacement in patients with severe aortic stenosis: a systematic review and meta-analysis.BMJ Open. 2021 Dec 6;11(12):e054222. doi: 10.1136/bmjopen-2021-054222. BMJ Open. 2021. PMID: 34873012 Free PMC article.
Cited by
-
Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association.Circulation. 2023 Feb 21;147(8):e93-e621. doi: 10.1161/CIR.0000000000001123. Epub 2023 Jan 25. Circulation. 2023. PMID: 36695182 Free PMC article. Review.
-
Comparison of infective endocarditis risk between balloon and self-expandable valves following transcatheter aortic valve replacement: systematic review and meta-analysis.Cardiovasc Interv Ther. 2021 Jul;36(3):363-374. doi: 10.1007/s12928-020-00675-1. Epub 2020 May 24. Cardiovasc Interv Ther. 2021. PMID: 32448938
-
2023 Korean Society of Echocardiography position paper for diagnosis and management of valvular heart disease, part I: aortic valve disease.J Cardiovasc Imaging. 2024 Jul 26;32(1):11. doi: 10.1186/s44348-024-00019-0. J Cardiovasc Imaging. 2024. PMID: 39061115 Free PMC article. Review.
-
Implications for prosthesis selection in dialysis patients undergoing aortic valve replacement.Gen Thorac Cardiovasc Surg. 2025 Feb;73(2):123-124. doi: 10.1007/s11748-024-02104-z. Epub 2024 Nov 13. Gen Thorac Cardiovasc Surg. 2025. PMID: 39538064 No abstract available.
-
Predictors of Permanent Pacemaker Implantation in Patients Undergoing Transcatheter Aortic Valve Replacement - A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2021 Jul 20;10(14):e020906. doi: 10.1161/JAHA.121.020906. Epub 2021 Jul 14. J Am Heart Assoc. 2021. PMID: 34259045 Free PMC article.
References
-
- Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease(version 2012):the Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur J Cardiothorac Surg 2012;42:S1-44. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous