

Mechanical versus bioprosthetic valves in patients on dialysis
- PMID: 31285893
- PMCID: PMC6588780
- DOI: 10.21037/jtd.2019.04.96
Mechanical versus bioprosthetic valves in patients on dialysis
Abstract
Background: The aim of this study is to evaluate the outcomes of bioprosthetic versus mechanical valves in patients on dialysis.
Methods: All patients who underwent aortic (AVR) or mitral valve replacement (MVR) at a single institution from 2011-2017 were reviewed. Primary stratification was bioprosthetic versus mechanical valves. The primary outcome was all-cause mortality. Secondary outcomes included hospital readmission, valve reoperation rates and bleeding events. Kaplan-Meier curves were generated and Cox proportional hazards regression models were used for risk-adjustment.
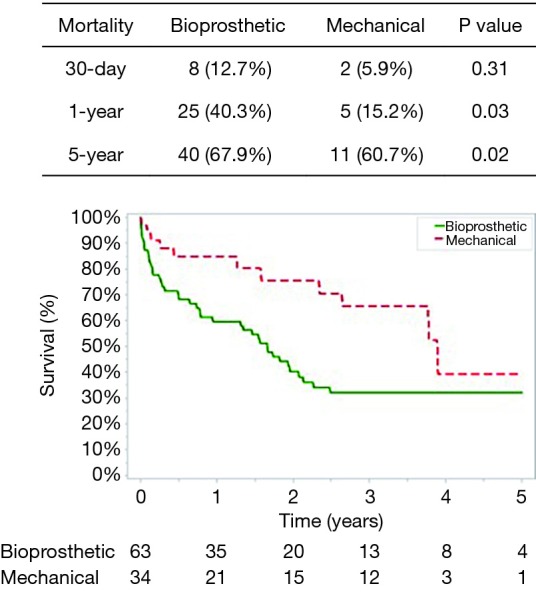
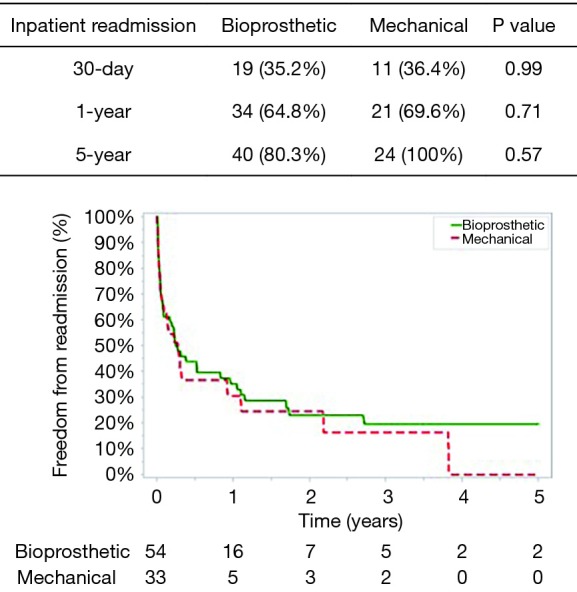
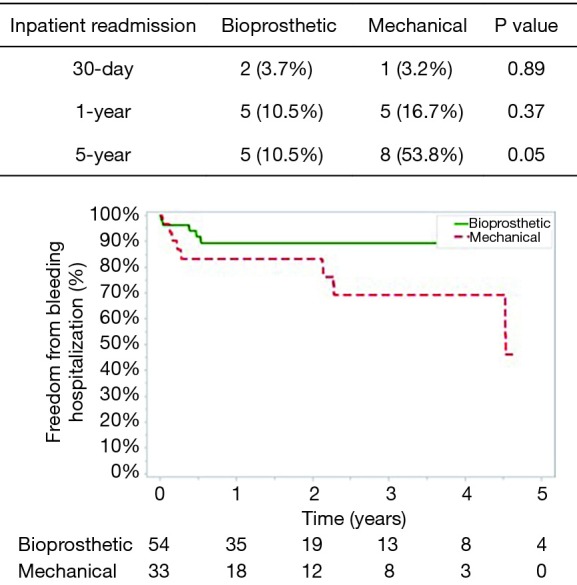
Results: During the study period, 3,969 patients underwent AVR or MVR, of which 97 (2.4%) were on dialysis. In dialysis patients, unadjusted 30-day mortality was comparable between bioprosthetic (12.7%) versus mechanical (5.9%) valves (P=0.31). However, the bioprosthetic group had higher rates of 1-year (40.3% versus 15.2%; P=0.03) and 5-year mortality (67.9% versus 60.7%; P=0.02). Most patients were readmitted within 5 years with no differences between the groups (bioprosthetic 80.3% versus mechanical 100%; P=0.57). There were no valve reoperations in either group at 5 years. The 5-year readmission rate was higher in the mechanical cohort (10.5% versus 53.8%; P=0.05). Risk-adjusted analysis confirmed these findings, where mechanical valves were independently associated with reduced mortality at 1-year and 5-years.
Conclusions: Despite the limited life expectancy of patients on dialysis, mechanical valves have an intermediate term mortality benefit compared to bioprosthetic valves. This comes at the expense of a higher rate of readmission for bleeding. Although valve choice should consider multiple factors, these data suggest that mechanical valve usage in dialysis patients is reasonable.
Keywords: Dialysis; aortic valve; mitral valve; survival; valve replacement.
Conflict of interest statement
Conflicts of Interest: TG Gleason—Medical Advisory Board, Abbott; A Kilic—Medical Advisory Board, Medtronic, Inc.The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Long-Term Outcomes of Bioprosthetic and Mechanical Valve Replacement for Patients Aged between 50 and 70 Years.Rev Cardiovasc Med. 2023 Sep 18;24(9):253. doi: 10.31083/j.rcm2409253. eCollection 2023 Sep. Rev Cardiovasc Med. 2023. PMID: 39076400 Free PMC article.
-
Outcomes of Surgical Mitral and Aortic Valve Replacements Among Kidney Transplant Candidates: Implications for Valve Selection.J Am Heart Assoc. 2021 Feb;10(5):e018971. doi: 10.1161/JAHA.120.018971. Epub 2021 Feb 18. J Am Heart Assoc. 2021. PMID: 33599143 Free PMC article.
-
Mechanical versus bioprosthetic valve replacement in middle-aged patients.Eur J Cardiothorac Surg. 2006 Sep;30(3):485-91. doi: 10.1016/j.ejcts.2006.06.013. Epub 2006 Jul 20. Eur J Cardiothorac Surg. 2006. PMID: 16857373
-
Mechanical Versus Bioprosthetic Valve Replacement in the Tricuspid Valve Position: A Systematic Review and Meta-Analysis.Heart Lung Circ. 2021 Mar;30(3):362-371. doi: 10.1016/j.hlc.2020.03.011. Epub 2020 Apr 1. Heart Lung Circ. 2021. PMID: 33229238
-
A systematic review on durability and structural valve deterioration in TAVR and surgical AVR.Acta Cardiol. 2021 Nov;76(9):921-932. doi: 10.1080/00015385.2020.1858250. Epub 2020 Dec 11. Acta Cardiol. 2021. PMID: 33302806
Cited by
-
Valve positions upon which cardiac surgeons operate should be taken into consideration.Can J Surg. 2023 Sep 6;66(5):E472-E473. doi: 10.1503/cjs.010122-l. Print 2023 Sep-Oct. Can J Surg. 2023. PMID: 37673440 Free PMC article. No abstract available.
-
Mechanical versus bioprosthetic valves in chronic dialysis: a systematic review and meta-analysis.Can J Surg. 2022 Jul 12;65(4):E450-E459. doi: 10.1503/cjs.001121. Print 2022 Jul-Aug. Can J Surg. 2022. PMID: 35820696 Free PMC article.
References
-
- United States Renal Data System. 2017 USRDS annual data report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2017.
LinkOut - more resources
Full Text Sources