

Editorial
doi: 10.21037/jtd.2018.12.128.
Perspective on airway stenting in inoperable patients with tracheoesophageal fistula after curative-intent treatment for esophageal cancer
Affiliations
- PMID: 31285911
- PMCID: PMC6588737
- DOI: 10.21037/jtd.2018.12.128
Item in Clipboard
Editorial
Perspective on airway stenting in inoperable patients with tracheoesophageal fistula after curative-intent treatment for esophageal cancer
J Thorac Dis.
2019 May.
No abstract available
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
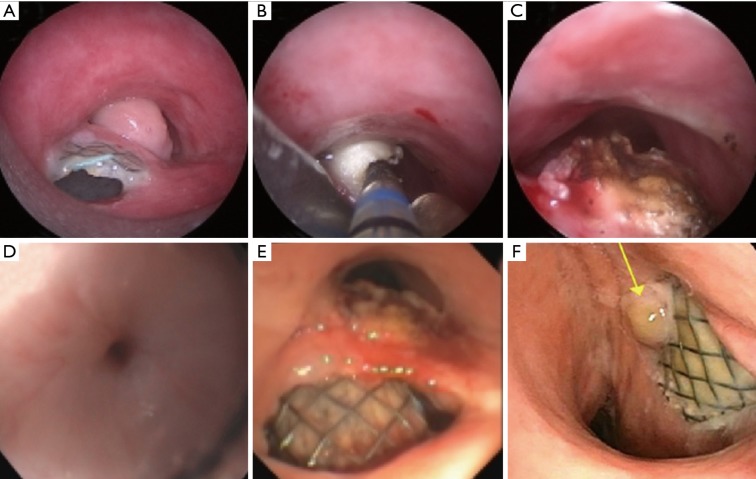
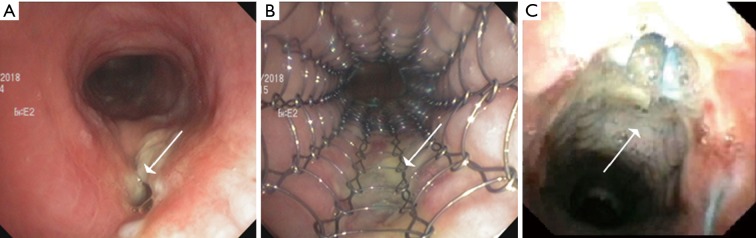
Patient with esophageal cancer who underwent esophageal stenting for a stricture and TEF following chemoradiotherapy. Six months later the esophageal stent had migrated caudally and eroded into the posterior tracheal wall causing a mass-like granulation tissue that obstructed 90% of the tracheal lumen (A). Electrosurgery (notice the white, coagulated color of the granulation tissue) and debulking was performed using CoreCath 2.7S (Medtronic Advanced Energy LLC; Portsmouth, NH) (B) to relieve the obstruction (C). There was a proximal esophageal stenosis (D) that permitted passage of only the pediatric endoscope, though which the esophageal stent was pulled up into optimal position (E) and balloon dilated. There was no contrast dye leak into the trachea on an esophagram and the patient had a significant improvement in symptoms. Bronchoscopy 1 month later showed continued coverage of the TEF by the fully expanded esophageal stent (F) with small granulation tissue (yellow arrow).
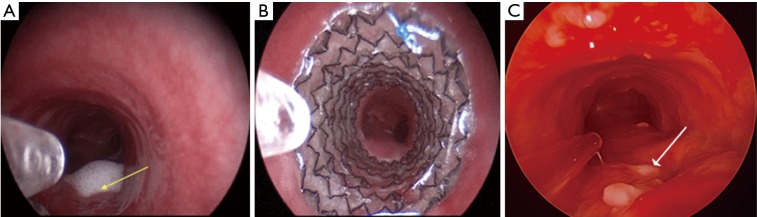
Patient with TGF (yellow arrow; evidenced by secretions leaking into the trachea) after an esophagectomy and gastric pull up surgery for esophageal cancer (A). The fistula was successfully covered by a tracheal fully covered SEMS (Merit Endotek) (B). One months later, the stent was removed as the fistula had completely healed (white arrow pointing at scar tissue) (C). TGF, tracheo-gastric fistula.
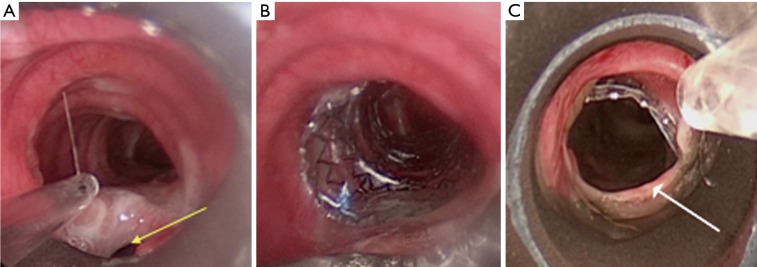
Patient with a high tracheal TEF (yellow arrow) 3 cm below the vocal cords (A). Esophageal stenting caused severe airway compression which could not be resolved optimally by stent resizing or repositioning, so the stent was removed. Given the proximity of the fistula to the subglottic region, a fully covered rather than partially covered tracheal SEMS (Merit Endotek) was placed to cover the fistula (B). The next day, the stent migrated caudally, protruding into the TEF posteriorly (as evidenced by the ridge of mucosa, i.e., posterior membrane; white arrow) (C). TEF, tracheoesophageal fistula.
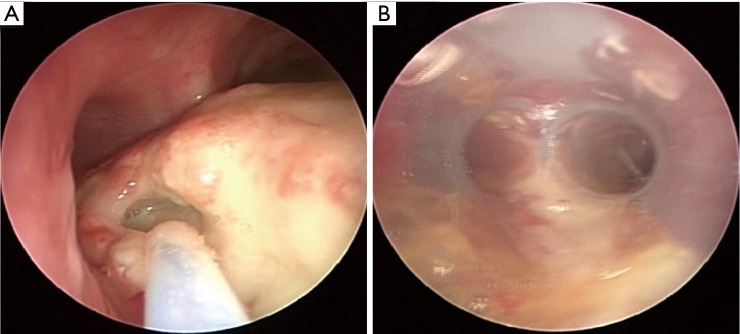
Patient with esophageal cancer who following chemoradiotherapy developed a 2 cm TEF in the distal trachea extending into the proximal left main bronchus (A). Due to concern for airway compression from planned esophageal stenting, an airway stent was inserted as the first step. A silicone Y Duman stent was chosen due to the location of the fistula (B).
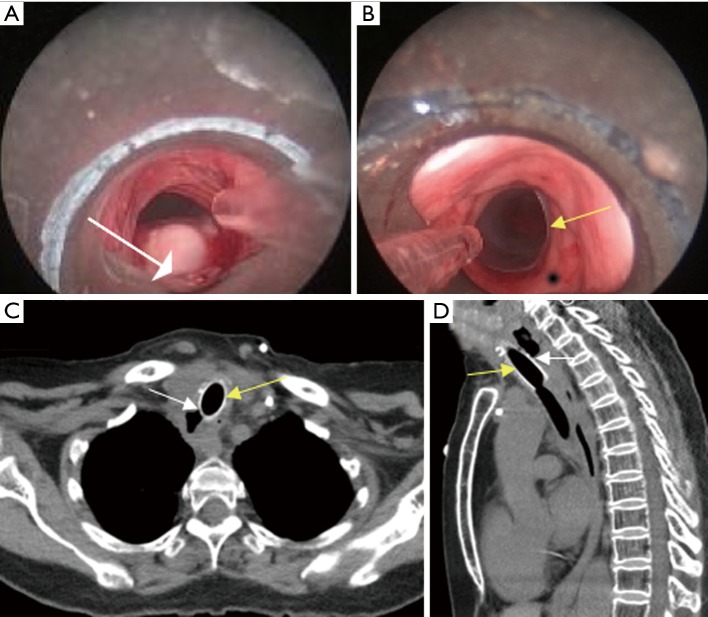
Patient with esophageal carcinoma treated with chemoradiotherapy, complicated by an upper tracheal TEF (A, white arrow) for which she received a partially covered SEMS (Ultraflex, Boston Scientific; Natick, MA, USA) that covered the fistula (B, white arrow). Esophageal stent could not be placed due to a severe proximal esophageal stenosis. Patient had significant initial improvement in symptoms. Inspection bronchoscopy 6 weeks later showed stable stent position and TEF occlusion with no granulation tissue (C, white arrow).
Patient with esophageal carcinoma who developed a TEF (white arrow) several months after chemoradiotherapy (A). Due to unsuccessful attempts at esophageal stent placement, a straight studded silicone stent was inserted in the trachea (B). Axial (C) and sagittal (D) CT scan 1 month later demonstrated stable stent position (yellow arrow) covering the TEF (white arrow). TEF, tracheoesophageal fistula.
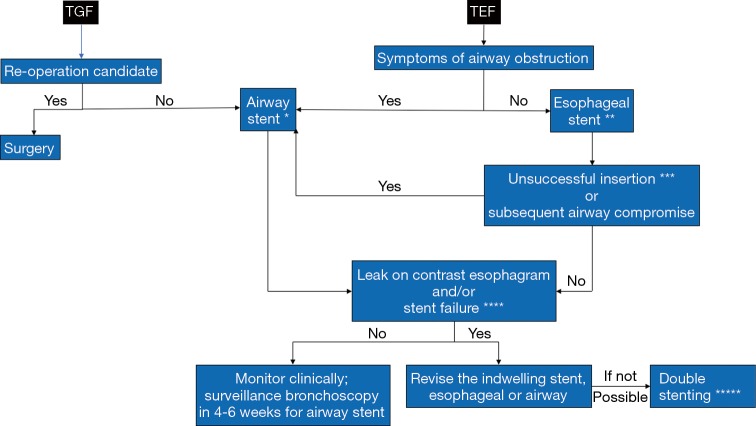
Algorithm to manage patients with TGF post esophagectomy and TEF post chemoradiotherapy for esophageal cancer. *, Decision to insert a silicone, fully covered SEMS or partially covered SEMS will depend on presence or absence of obstruction, degree of obstruction, and location of fistula; **, if a clinician suspects airway compromise post esophageal stenting, a flexible bronchoscopy or computed tomography scan is recommended to detect the degree of airway compromise. In case a patient develops symptoms of airway obstruction, either revision of the esophageal stent or insertion of an airway stent should be performed. Occasionally the clinician may predict airway compromise post esophageal stenting, in which case an airway stent may be inserted as a first step. This is uncommon post chemoradiotherapy as there is no tumor to compress the airway; ***, stent inserted but did not deploy optimally, or insertion was not possible due to concurrent esophageal stricture; ****, bronchoscopic or endoscopic persistent fistula despite stenting, or stent migration; *****, this practice poses the risk for enlargement of the fistula and is not recommended in patients who may become surgical candidates.
Similar articles
-
Airway ultraflex stenting in esophageal cancer with esophagorespiratory fistula.Am J Med Sci. 2012 Aug;344(2):105-9. doi: 10.1097/MAJ.0b013e3182367b6a. Am J Med Sci. 2012. PMID: 22143123
-
Management of malignant esophagotracheal fistulas with airway stenting and double stenting.Chest. 1996 Nov;110(5):1155-60. doi: 10.1378/chest.110.5.1155. Chest. 1996. PMID: 8915213
-
The treatment strategy for tracheoesophageal fistula.J Thorac Dis. 2015 Dec;7(Suppl 4):S389-97. doi: 10.3978/j.issn.2072-1439.2015.12.11. J Thorac Dis. 2015. PMID: 26807286 Free PMC article. Review.
-
[Usefulness of esophageal stenting for esophagorespiratory fistula with esophageal cancer].Gan To Kagaku Ryoho. 2012 Nov;39(12):1849-51. Gan To Kagaku Ryoho. 2012. PMID: 23267907 Japanese.
-
[Interventional treatment of tracheoesophageal/bronchoesophageal fistulas].Chirurg. 2019 Sep;90(9):710-721. doi: 10.1007/s00104-019-0988-z. Chirurg. 2019. PMID: 31240352 Review. German.
Cited by
-
Palliative management of a malignant tracheoesophageal fistula using repeat endobronchial laser debridement and esophageal stenting.J Surg Case Rep. 2023 Dec 30;2023(12):rjad590. doi: 10.1093/jscr/rjad590. eCollection 2023 Dec. J Surg Case Rep. 2023. PMID: 38164211 Free PMC article.
-
Silicone stent versus fully covered metallic stent in tracheoesophageal fistula: a single-center retrospective study.BMC Pulm Med. 2024 Dec 18;24(1):612. doi: 10.1186/s12890-024-03434-7. BMC Pulm Med. 2024. PMID: 39696272 Free PMC article.
-
Endoluminal Wound Vacuum Therapy: A Paradigm Shift in Managing Esophageal Bronchial Fistula.Ann Thorac Surg Short Rep. 2024 Jul 25;2(4):703-706. doi: 10.1016/j.atssr.2024.07.004. eCollection 2024 Dec. Ann Thorac Surg Short Rep. 2024. PMID: 39790607 Free PMC article.
-
Efficacy of airway stenting and nasogastric tube insertion in airway-esophageal fistula patients with airways compromised by advanced malignancy.Clin Respir J. 2024 Feb;18(2):e13737. doi: 10.1111/crj.13737. Clin Respir J. 2024. PMID: 38350674 Free PMC article.
-
The clinical characteristics, treatments and prognosis of post-esophagectomy airway fistula: a multicenter cohort study.Transl Lung Cancer Res. 2022 Mar;11(3):331-341. doi: 10.21037/tlcr-22-141. Transl Lung Cancer Res. 2022. PMID: 35399570 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources