

Retrospective analysis into differences in heart failure patients with and without iron deficiency or anaemia
- PMID: 31286685
- PMCID: PMC6676442
- DOI: 10.1002/ehf2.12485
Retrospective analysis into differences in heart failure patients with and without iron deficiency or anaemia
Abstract
Aims: The aim of this study was to assess the burden of heart failure (HF) patients with/without iron deficiency/iron deficiency anaemia (ID/A) from the health insurance perspective.
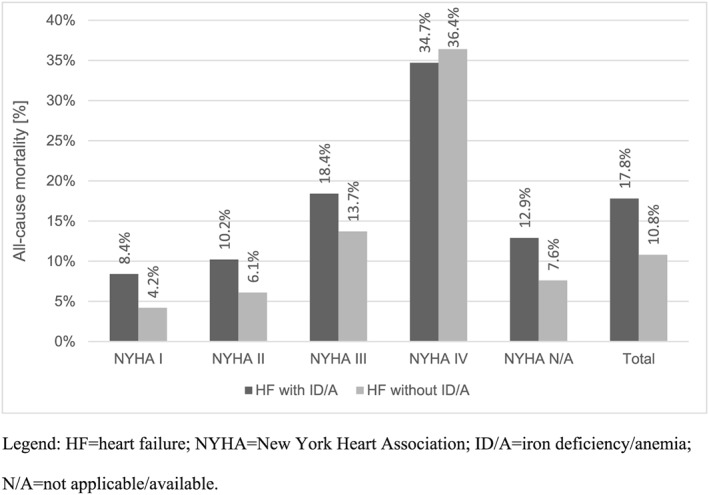
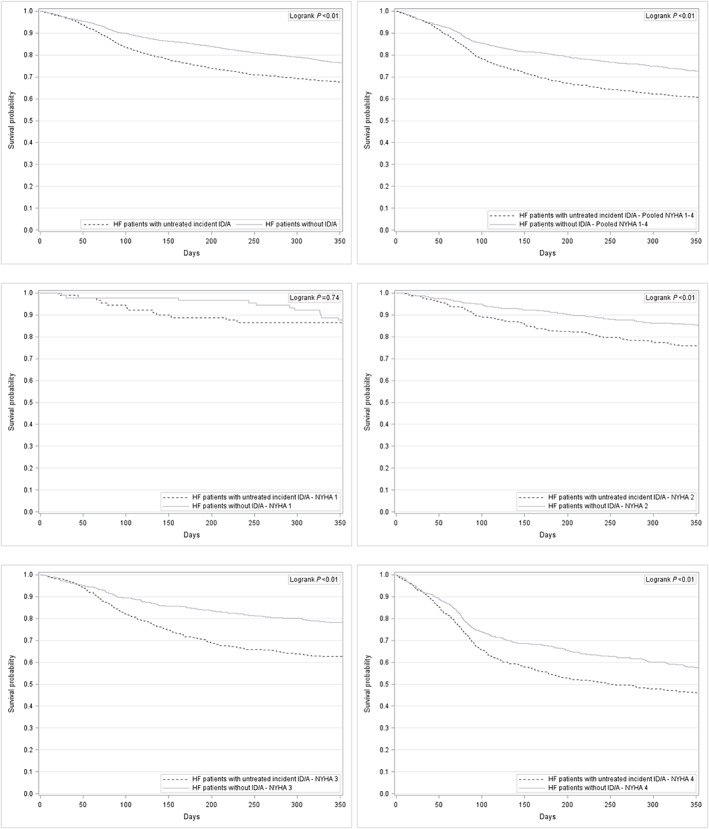
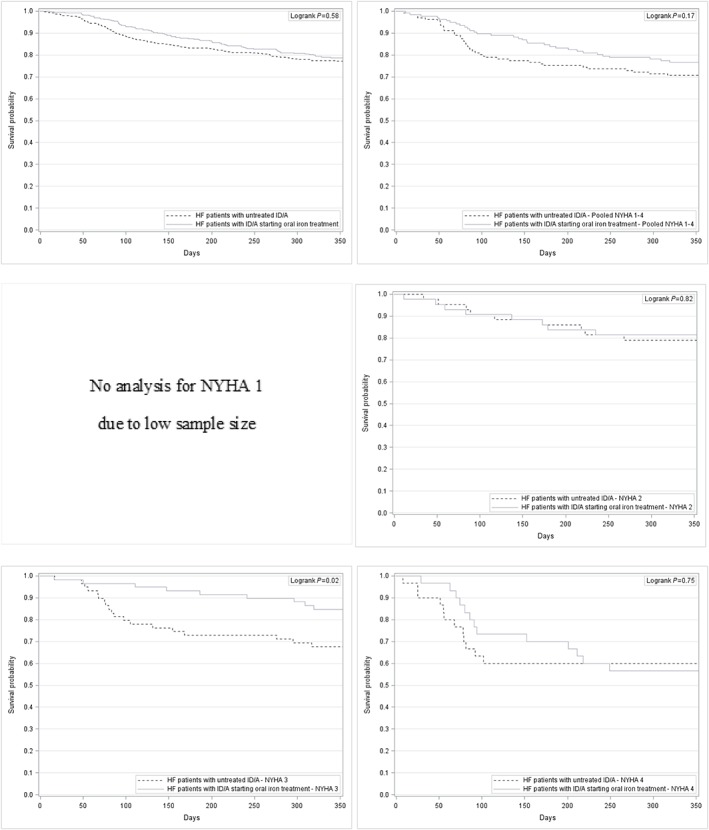
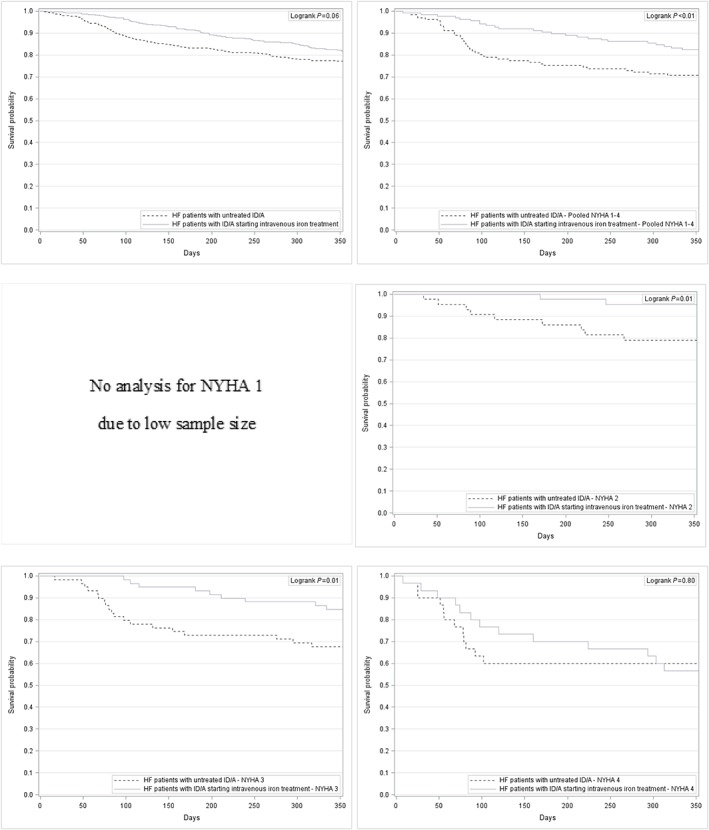
Methods and results: We conducted a retrospective claims database analysis using the Institut für angewandte Gesundheitsforschung Berlin research database. The study period spanned from 1 January 2012 to 31 December 2014. HF patients were identified by International Statistical Classification of Diseases and Related Health Problems, 10th revision, German Modification codes (I50.-, I50.0-, I50.00, I50.01, I50.1-, I50.11, I50.12, I50.13, I50.14, I50.19, and I50.9). HF patients were stratified into HF patients without ID/A and HF patients with ID/A (D50.-, D50.0, D50.8, D50.9, and E61.1). HF patients with ID/A were stratified into three subgroups: no iron treatment, oral iron treatment, and intravenous iron treatment. A matching approach was applied to compare outcomes for HF patients without ID/A vs. HF patient with untreated incident ID/A without iron treatment and for HF patients receiving no iron treatment vs. oral iron treatment vs. intravenous iron treatment. Matching parameters included exact age, sex, and New York Heart Association functional class. An optimization algorithm was used to balance total health care costs in the baseline period for the potential matched pairs without sample size reduction. In total, 172 394 (4537.4 per 100 000) HF patients were identified in the Institut für angewandte Gesundheitsforschung Berlin research database in 2013. Of these, 11.1% (19 070; 501.9 per 100 000) were diagnosed with ID/A and/or had a prescription for iron medication in 2013. The mean age of HF patients was 77.0 years (±12.0 years). Women were more frequently diagnosed with HF (54.6%). HF patients with untreated incident ID/A (1.77%) had a significantly higher all-cause mortality than HF patients without ID/A (33.1% vs. 24.1%, P < 0.01). The analysis of health care utilization revealed significant differences in the rate of all-cause hospitalization (72.9% vs. 50.5%, P < 0.01). The annual health care costs for HF patients with untreated incident ID/A amounted to €17 347 with incremental costs of €849 (P < 0.01) attributed to ID/A.
Conclusions: Heart failure is associated with a major burden for patients and the health care system in terms of health care resource utilization, costs, and mortality. Our findings suggest that there is an unmet need for treating more HF patients with ID/A with iron medication.
Keywords: Claims data; Cost of illness; Heart failure; Iron deficiency anaemia; Statutory health insurance.
© 2019 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
I.B. and T.H. are employees of Vifor Pharma and Vifor Fresenius Medical Care Renal Pharma, Munich, Germany. The authors declare that no further conflict of interest exists.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, ESC Scientific Document Group . ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Eur Heart J 2016; 37: 2129–2200. - PubMed
-
- The Criteria Committee of the New York Heart Association . Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels, 9th ed. Boston, Mass: Little, Brown & Co; 1994. 253–256.
-
- Deutsche Gesellschaft für Allgemeinmedizin und Familienmedizin (DEGAM) , Leitlinie Nr. 9: Herzinsuffizienz. Langfassung. Omikron Publ; 2006.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
