Clinical Usefulness of Intraoperative Motor-Evoked Potential Monitoring during Temporal Lobe Epilepsy Surgery
- PMID: 31286698
- PMCID: PMC6620456
- DOI: 10.3988/jcn.2019.15.3.285
Clinical Usefulness of Intraoperative Motor-Evoked Potential Monitoring during Temporal Lobe Epilepsy Surgery
Abstract
Background and purpose: We aimed to determine the effectiveness of intraoperative neurophysiological monitoring focused on the transcranial motor-evoked potential (MEP) in patients with medically refractory temporal lobe epilepsy (TLE).
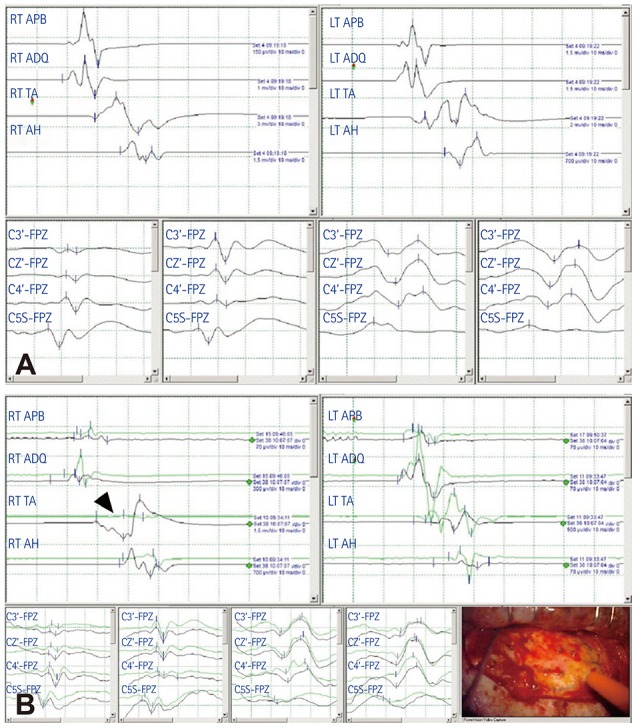
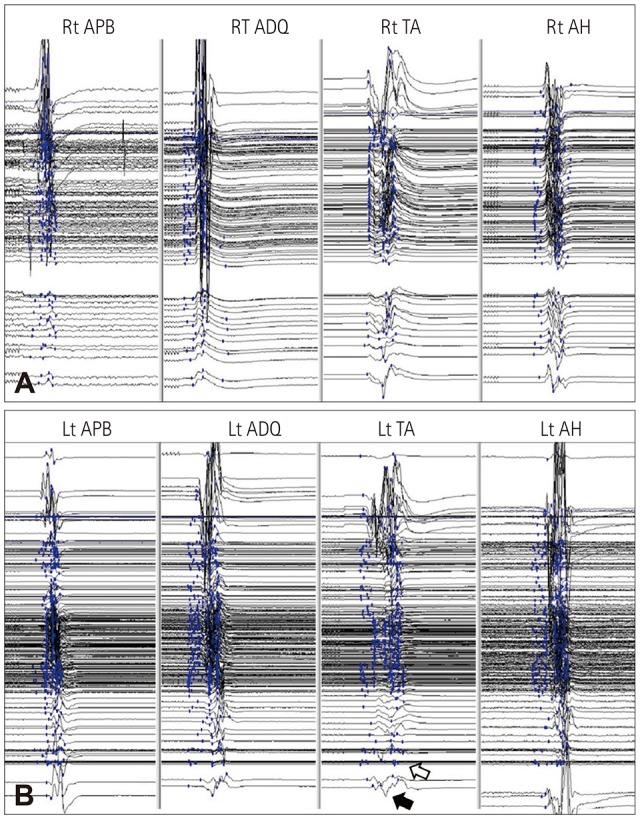
Methods: We compared postoperative neurological deficits in patients who underwent TLE surgery with or without transcranial MEPs combined with somatosensory evoked potential (SSEP) monitoring between January 1995 and June 2018. Transcranial motor stimulation was performed using subdermal electrodes, and MEP responses were recorded in the four extremity muscles. A decrease of more than 50% in the MEP or the SSEP amplitudes compared with baseline was used as a warning criterion.
Results: In the TLE surgery group without MEP monitoring, postoperative permanent motor deficits newly developed in 7 of 613 patients. In contrast, no permanent motor deficit occurred in 279 patients who received transcranial MEP and SSEP monitoring. Ten patients who exhibited decreases of more than 50% in the MEP amplitude recovered completely, although two cases showed transient motor deficits that recovered within 3 months postoperatively.
Conclusions: Intraoperative transcranial MEP monitoring during TLE surgery allowed the prompt detection and appropriate correction of injuries to the motor nervous system or ischemic stroke. Intraoperative transcranial MEP monitoring is a reliable modality for minimizing motor deficits in TLE surgery.
Keywords: intraoperative monitoring; motor-evoked potentials; temporal lobe epilepsy.
Copyright © 2019 Korean Neurological Association.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
Similar articles
-
[Evaluation of a Combination of Waveform Amplitude Latency and Decrease of Waveform Amplitude Magnitude during Spinal Surgery in Intraoperative Neurophysiological Monitoring of Transcranial Motor Evoked Potentials and Its Incidence on Postoperative Neurological Deficit].Acta Chir Orthop Traumatol Cech. 2020;87(1):39-47. Acta Chir Orthop Traumatol Cech. 2020. PMID: 32131970 Slovak.
-
Combined motor and somatosensory evoked potentials for intraoperative monitoring: intra- and postoperative data in a series of 69 operations.Neurosurg Rev. 2007 Apr;30(2):109-16; discussion 116. doi: 10.1007/s10143-006-0061-5. Epub 2007 Jan 13. Neurosurg Rev. 2007. PMID: 17221265 Clinical Trial.
-
Analysis of Multimodal Intraoperative Monitoring During Intramedullary Spinal Ependymoma Surgery.World Neurosurg. 2018 Dec;120:e169-e180. doi: 10.1016/j.wneu.2018.07.267. Epub 2018 Aug 8. World Neurosurg. 2018. PMID: 30096497
-
The Interpretation of Muscle Motor Evoked Potentials for Spinal Cord Monitoring.J Clin Neurophysiol. 2017 Jan;34(1):32-37. doi: 10.1097/WNP.0000000000000314. J Clin Neurophysiol. 2017. PMID: 28045855 Review.
-
Intraoperative neurophysiologic monitoring for intramedullary spinal-cord tumor surgery.Neurophysiol Clin. 2007 Dec;37(6):407-14. doi: 10.1016/j.neucli.2007.10.003. Epub 2007 Nov 9. Neurophysiol Clin. 2007. PMID: 18083496 Review.
Cited by
-
Motor Evoked Potential Warning Criteria in Supratentorial Surgery: A Scoping Review.Cancers (Basel). 2021 Jun 4;13(11):2803. doi: 10.3390/cancers13112803. Cancers (Basel). 2021. PMID: 34199853 Free PMC article.
References
-
- Wiebe S, Blume WT, Girvin JP, Eliasziw M Effectiveness and Efficiency of Surgery for Temporal Lobe Epilepsy Study Group. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med. 2001;345:311–318. - PubMed
-
- Engel J., Jr The timing of surgical intervention for mesial temporal lobe epilepsy: a plan for a randomized clinical trial. Arch Neurol. 1999;56:1338–1341. - PubMed
-
- Muzumdar D, Patil M, Goel A, Ravat S, Sawant N, Shah U. Mesial temporal lobe epilepsy–An overview of surgical techniques. Int J Surg. 2016;36:411–419. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources