

A mixed-methods evaluation of the MOREOB program in Ontario hospitals: participant knowledge, organizational culture, and experiences
- PMID: 31286979
- PMCID: PMC6615285
- DOI: 10.1186/s12913-019-4224-9
A mixed-methods evaluation of the MOREOB program in Ontario hospitals: participant knowledge, organizational culture, and experiences
Abstract
Background: MOREOB (Managing Obstetrical Risk Efficiently) is a patient safety program for health care providers and administrators in hospital obstetric units. MOREOB has been implemented widely in Canada and gradually spread to the United States. The main goal of MOREOB is to build a patient safety culture and improve clinical outcomes. In 2013, 26 Ontario hospitals voluntarily accepted provincial funding to participate in MOREOB. The purpose of our study was to assess the effect of MOREOB on participant knowledge, organizational culture, and experiences implementing and participating in the program at these 26 Ontario hospitals.
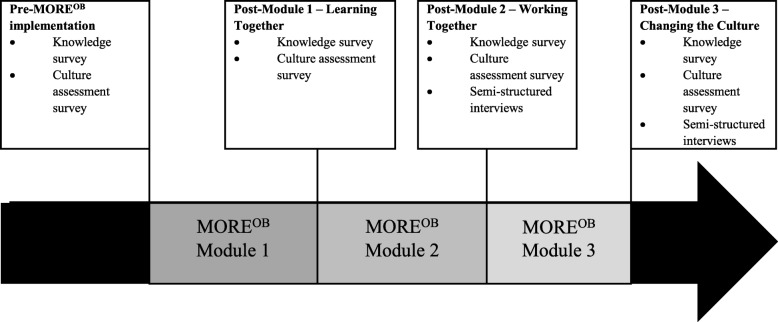
Methods: A convergent parallel mixed-methods study in Ontario, Canada, with MOREOB participants from 26 hospitals. The quantitative component used a descriptive pre-post repeated measures design to assess participant knowledge and perception of culture, administered pre-MOREOB and after each of the three MOREOB modules. Changes in mean scores were assessed using mixed-effects regression. The qualitative component used a qualitative descriptive design with individual semi-structured interviews. We used content analysis to code, categorize, and thematically describe data. A convergent parallel design was used to triangulate findings from data sources.
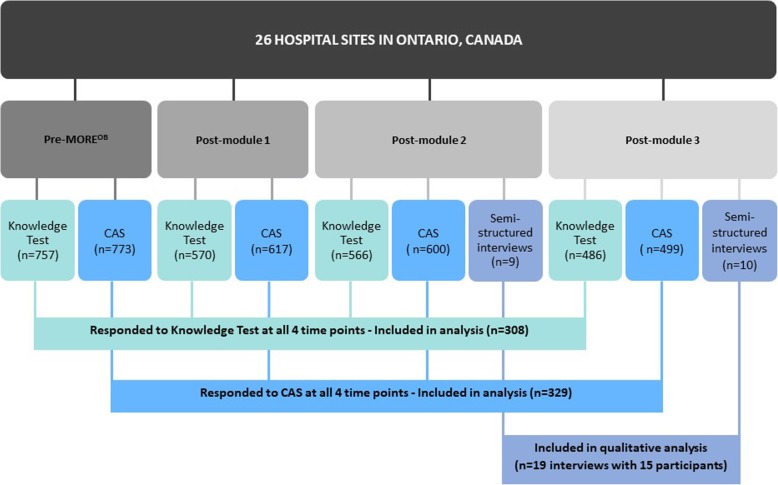
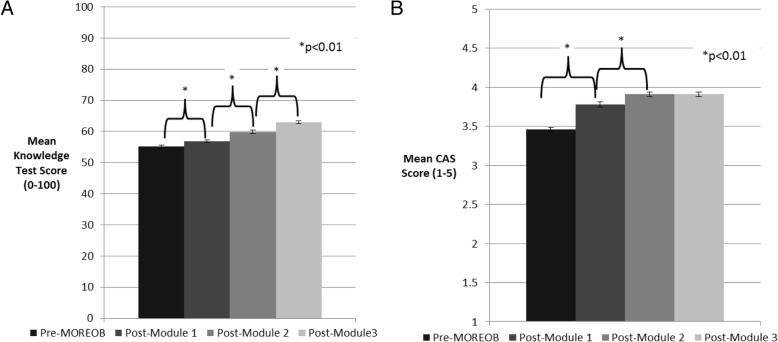
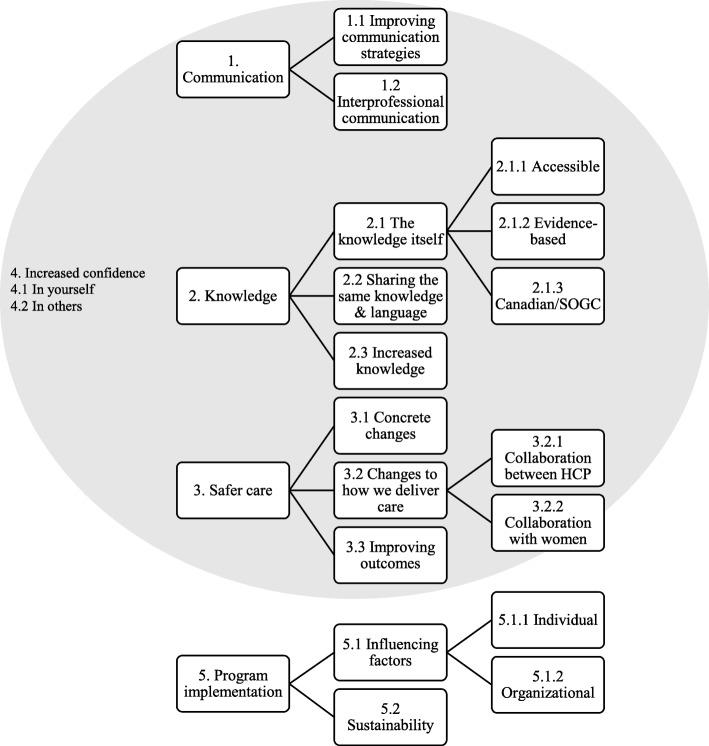
Results: 308 participants completed the knowledge test, and 329 completed the culture assessment at all four time points. Between baseline and post-Module 3, statistically significant increases on both scores were observed, with an increase of 7.9% (95% CI: 7.1 to 8.8) on the knowledge test and an increase of 0.45 (on a scale of 1-5, 95% CI: 0.38 to 0.52) on the culture assessment. Interview participants (n = 15) described improvements in knowledge, interprofessional communication, ability to provide safe care, and confidence in skills. Facilitators and barriers to program implementation and sustainability were identified.
Conclusions: Participants were satisfied with their participation in the MOREOB program and perceived that it increased health care provider knowledge and confidence, improved safety for patients, and improved communication between team members. Additionally, mean scores on knowledge tests for obstetric content and culture assessment improved. The MOREOB program can help organizations and individuals improve care by concentrating on the human and organizational aspects of patient safety. Further work to improve program implementation and sustainability is required.
Keywords: Obstetrics and gynecology; Patient safety; Qualitative research; Safety culture; Surveys.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Statistics Canada. Births, 2015 and 2016. Ottawa; 2018. https://www150.statcan.gc.ca/n1/en/daily-quotidien/180430/dq180430f-eng..... Accessed 12 June 2019.
-
- Canadian Institute of Health Information (CIHI). Giving birth in Canada: a regional profile. Ottawa; 2004. https://secure.cihi.ca/free_products/GBC2004_regional_e.pdf. Accessed 8 Apr 2019
-
- Public Health Agency of Canada. Perinatal health indicators for Canada 2017. Ottawa; 2017. http://publications.gc.ca/collections/collection_2018/aspc-phac/HP7-1-20.... Accessed 8 Apr 2019.
-
- Kohn LT, Corrigan JM, Donaldson MS. To err is human: building a safer health system. Washington, DC: National Academy Press; 1999. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
