

Diffusion weighted cardiovascular magnetic resonance imaging for discriminating acute from non-acute deep venous Thrombus
- PMID: 31286985
- PMCID: PMC6615231
- DOI: 10.1186/s12968-019-0552-5
Diffusion weighted cardiovascular magnetic resonance imaging for discriminating acute from non-acute deep venous Thrombus
Abstract
Background: The importance of discriminating acute from non-acute thrombus is highlighted. The study aims to investigate the feasibility of readout-segmented diffusion weighted (DW) cardiovascular magnetic resonance (CMR) for discrimination of acute from non-acute deep venous thrombus (DVT).
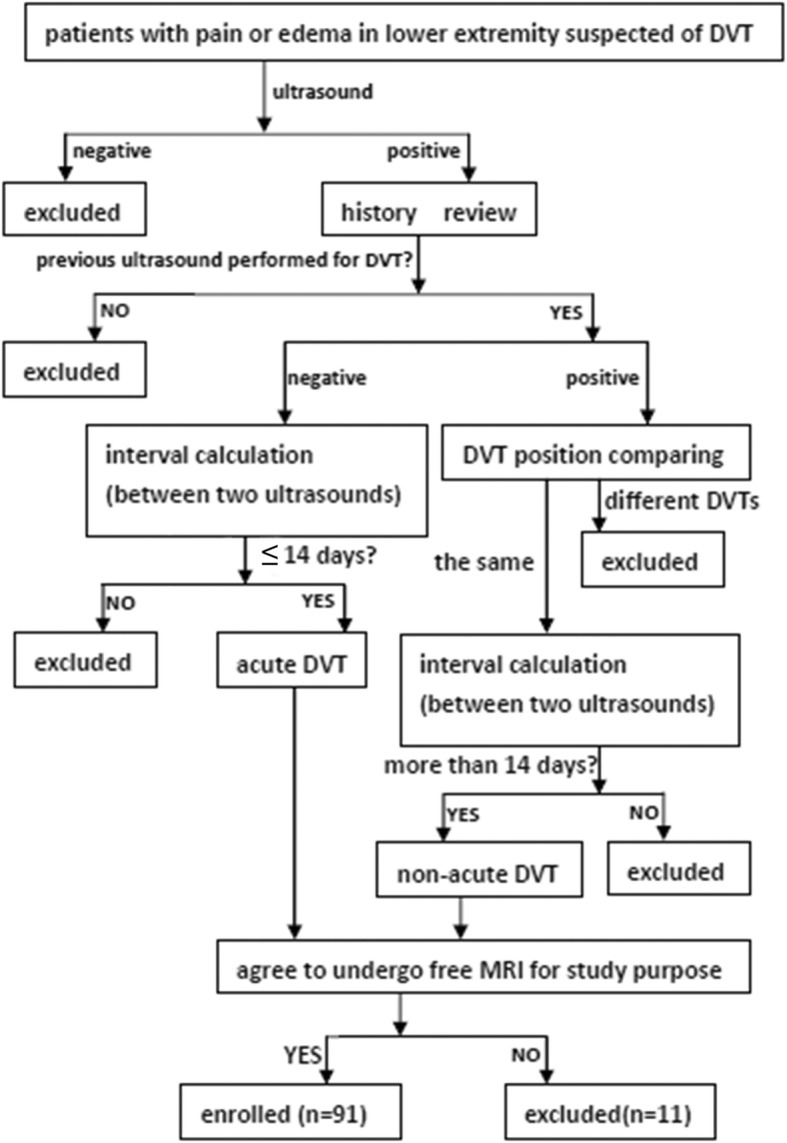
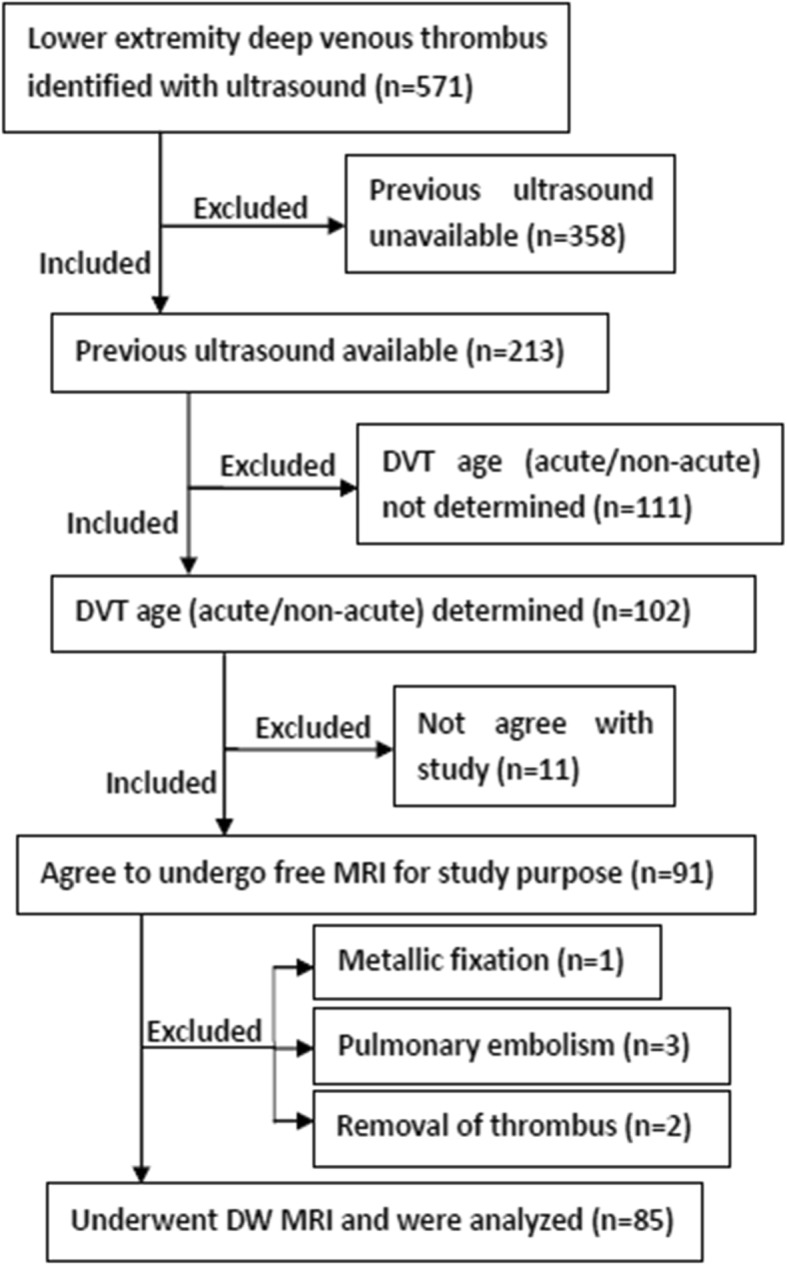
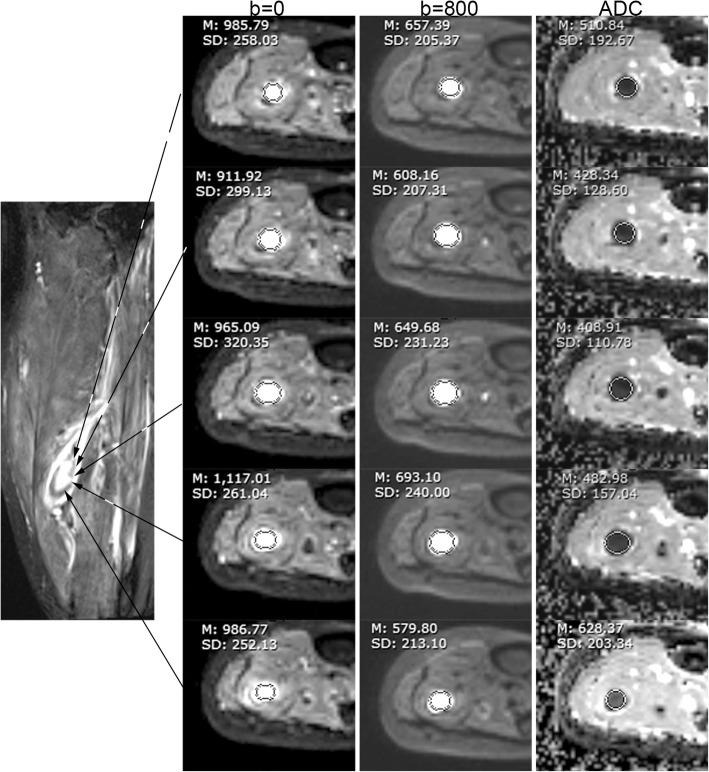
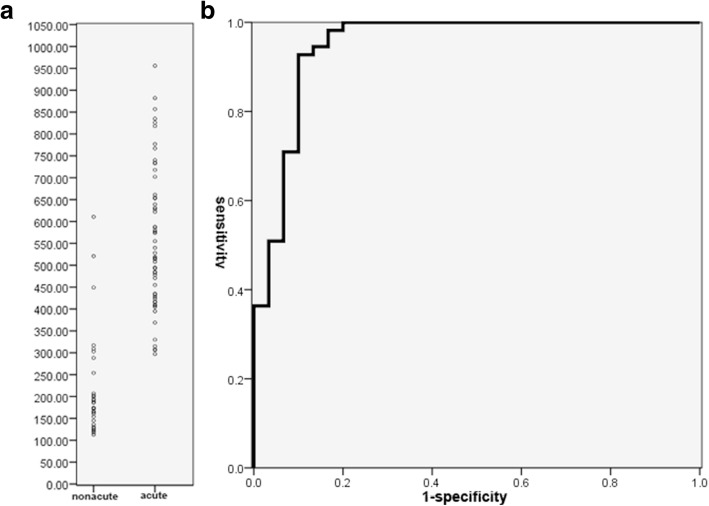
Methods: For this prospective study from December 2015 to December 2017, 85 participants (mean age = 53 years, age range = 34~74) with DVT of lower extremities underwent readout-segmented DW CMR. DVT of ≤14 days were defined as acute (n = 55) and > 14 days as non-acute (n = 30). DVT visualization on b = 0, b = 800, and apparent diffusion coefficient (ADC) images were assessed using a 4-point scale (0~3, poor~excellent). DW CMR parameters were measured using region of interest (ROI). Relative signal intensity (rSI) and ADC were compared between acute and non-acute DVT using a Mann Whitney test. Sensitivity and specificity for ADC and rSI were calculated.
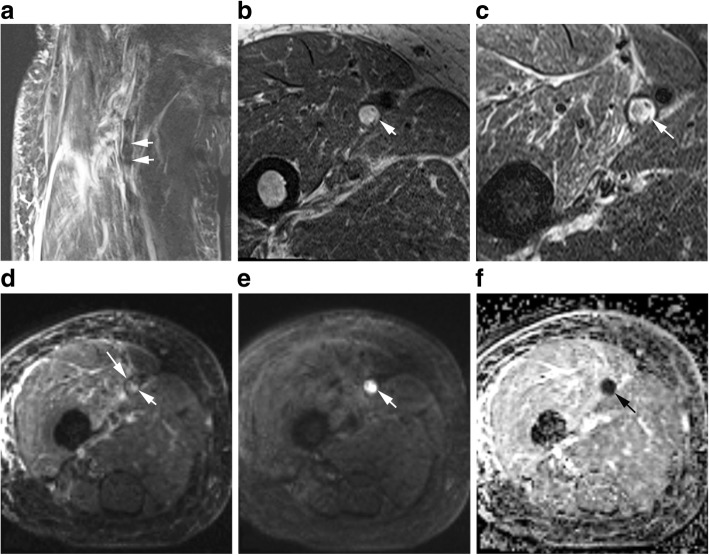
Results: ADC maps had higher visualization scores than b = 0 and b = 800 images (2.7 ± 0.5, 2.5 ± 0.6, and 2.4 ± 0.6 respectively, P<0.05). The mean ADC was higher in acute DVT than non-acute DVT (0.56 ± 0.17 × 10- 3 vs. 0.22 ± 0.12 × 10- 3 mm2/s, P<0.001). Using 0.32 × 10- 3 mm2/s as the cutoff, sensitivity and specificity for ADC to discriminate acute from non-acute DVT were 93 and 90% respectively. Sensitivity and specificity were 73 and 60% for rSI on b = 0, and 75 and 63% for rSI on b = 800.
Conclusions: Readout segmented diffusion-weighted CMR derived ADC distinguishes acute from non-acute DVT.
Trial registration: This study is retrospectively registered.
Trial registration number: HUST-TJH-2015-146 .
Keywords: Apparent diffusion coefficient; Diffusion; MRI; Thrombus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
T1 mapping is useful for staging deep venous thrombosis in the lower extremities.Acta Radiol. 2022 Apr;63(4):489-496. doi: 10.1177/02841851211004425. Epub 2021 Apr 28. Acta Radiol. 2022. PMID: 33910379
-
Black-blood thrombus imaging (BTI): a contrast-free cardiovascular magnetic resonance approach for the diagnosis of non-acute deep vein thrombosis.J Cardiovasc Magn Reson. 2017 Jan 18;19(1):4. doi: 10.1186/s12968-016-0320-8. J Cardiovasc Magn Reson. 2017. PMID: 28095878 Free PMC article.
-
Chemical-shift and diffusion-weighted magnetic resonance imaging of thymus in myasthenia gravis: usefulness of quantitative assessment.Invest Radiol. 2015 Apr;50(4):228-38. doi: 10.1097/RLI.0000000000000120. Invest Radiol. 2015. PMID: 25478741
-
Cardiovascular magnetic resonance black-blood thrombus imaging for the diagnosis of acute deep vein thrombosis at 1.5 Tesla.J Cardiovasc Magn Reson. 2018 Jun 25;20(1):42. doi: 10.1186/s12968-018-0459-6. J Cardiovasc Magn Reson. 2018. PMID: 29936910 Free PMC article.
-
Differentiation of malignant thrombus from bland thrombus of the portal vein in patients with hepatocellular carcinoma: application of diffusion-weighted MR imaging.Radiology. 2010 Jan;254(1):154-62. doi: 10.1148/radiol.09090304. Radiology. 2010. PMID: 20032150
Cited by
-
High Signal Intensity on Diffusion-Weighted Images Reflects Acute Phase of Deep Vein Thrombus.Thromb Haemost. 2020 Oct;120(10):1463-1473. doi: 10.1055/s-0040-1714280. Epub 2020 Aug 3. Thromb Haemost. 2020. PMID: 32746467 Free PMC article.
-
Diffusion-Weighted Imaging Prior to Percutaneous Sclerotherapy of Venous Malformations-Proof of Concept Study for Prediction of Clinical Outcome.Diagnostics (Basel). 2022 Jun 9;12(6):1430. doi: 10.3390/diagnostics12061430. Diagnostics (Basel). 2022. PMID: 35741240 Free PMC article.
-
Magnetic resonance (MR) evaluation of deep venous thrombosis of 338 discharged viral pneumonia patients.Quant Imaging Med Surg. 2024 Sep 1;14(9):6413-6424. doi: 10.21037/qims-23-1607. Epub 2024 Aug 28. Quant Imaging Med Surg. 2024. PMID: 39281170 Free PMC article.
-
Signal Change of Jugular Vein Thrombus on Diffusion-Weighted Magnetic Resonance Imaging.Circ Rep. 2020 Jul 15;2(8):455-456. doi: 10.1253/circrep.CR-20-0039. Circ Rep. 2020. PMID: 33693269 Free PMC article. No abstract available.
References
-
- Naess IA, Christiansen SC, Romundstad P, et al. Incidence and mortality of venous thrombosis: a population-based study. JTH. 2007;5:692–699. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
