

Persistent Hotspots in Schistosomiasis Consortium for Operational Research and Evaluation Studies for Gaining and Sustaining Control of Schistosomiasis after Four Years of Mass Drug Administration of Praziquantel
- PMID: 31287046
- PMCID: PMC6726953
- DOI: 10.4269/ajtmh.19-0193
Persistent Hotspots in Schistosomiasis Consortium for Operational Research and Evaluation Studies for Gaining and Sustaining Control of Schistosomiasis after Four Years of Mass Drug Administration of Praziquantel
Abstract
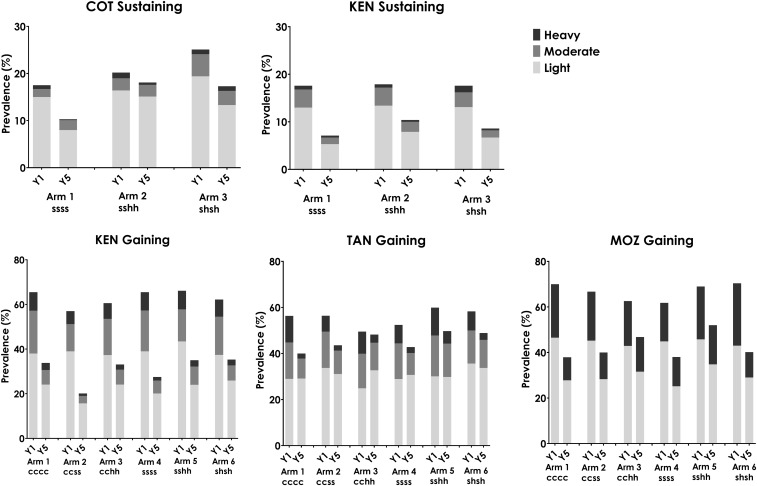
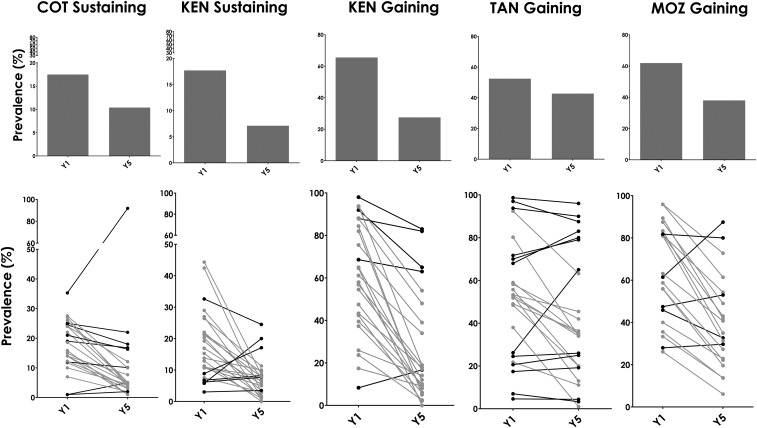
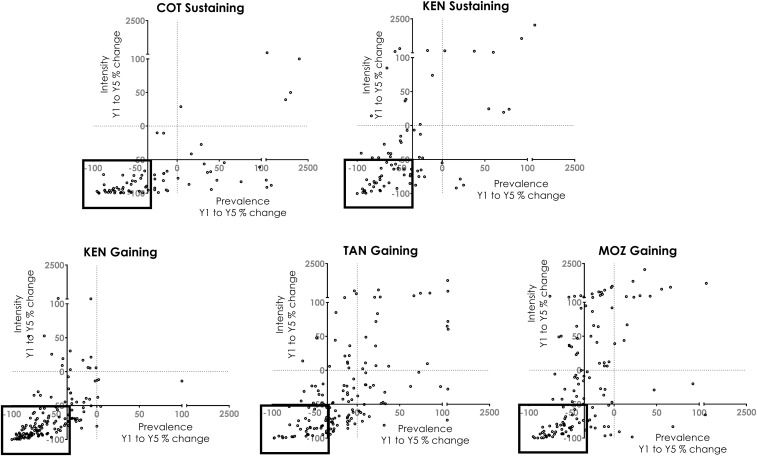
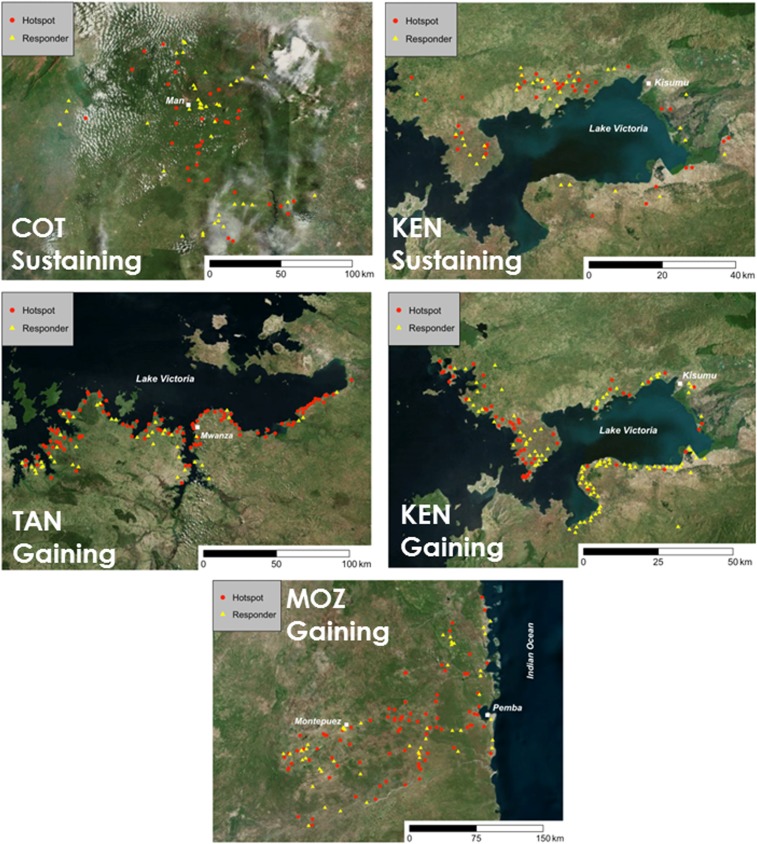
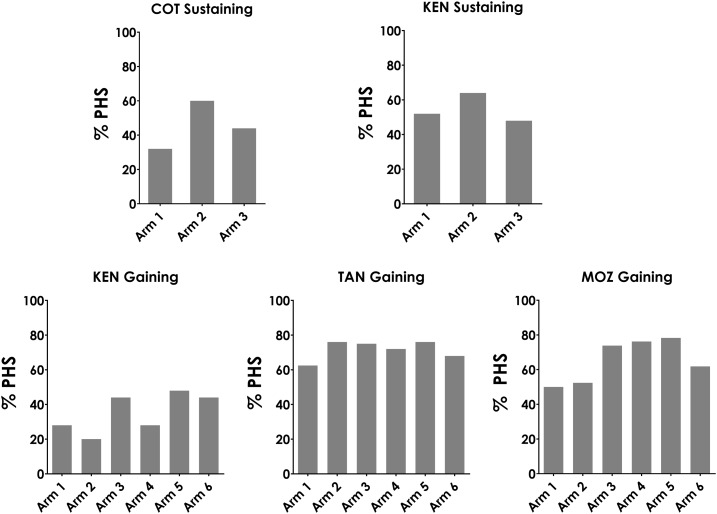
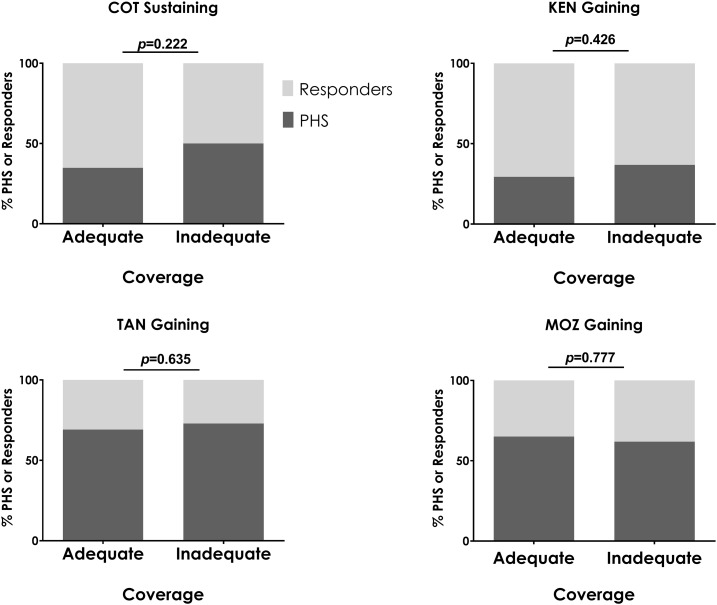
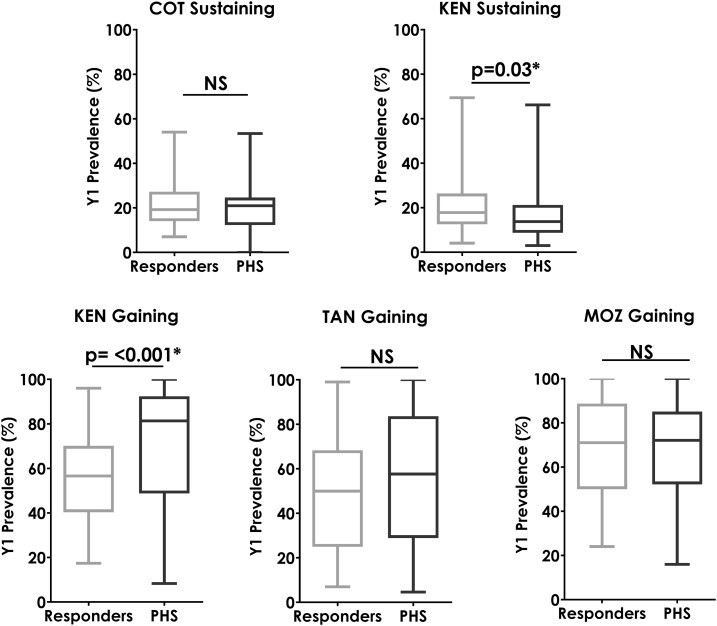
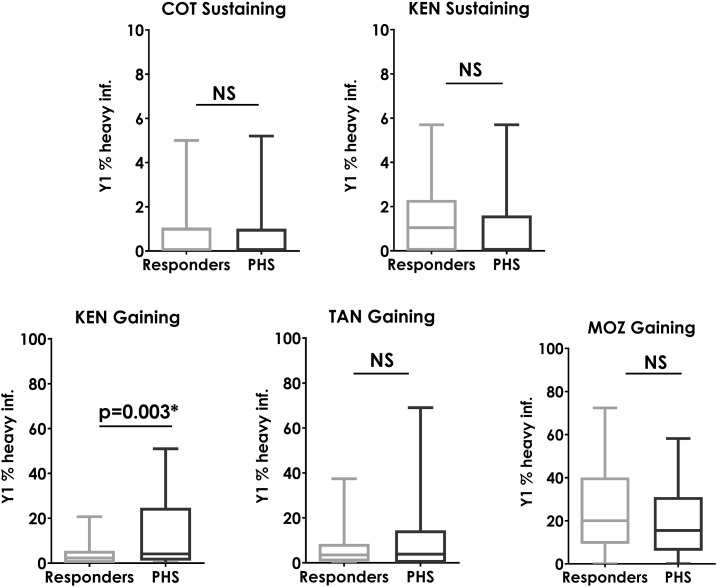
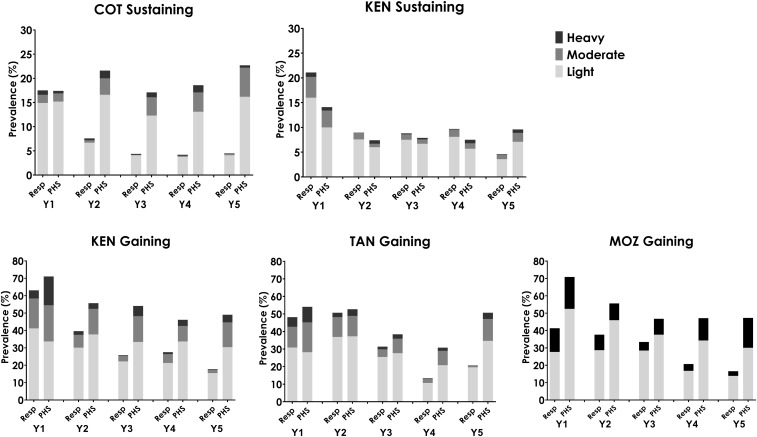
Control of schistosomiasis presently relies largely on preventive chemotherapy with praziquantel through mass drug administration (MDA) programs. The Schistosomiasis Consortium for Operational Research and Evaluation has concluded five studies in four countries (Côte d'Ivoire, Kenya, Mozambique, and Tanzania) to evaluate alternative approaches to MDA. Studies involved four intervention years, with final evaluation in the fifth year. Mass drug administration given annually or twice over 4 years reduced average prevalence and intensity of schistosome infections, but not all villages that were treated in the same way responded similarly. There are multiple ways by which responsiveness to MDA, or the lack thereof, could be measured. In the analyses presented here, we defined persistent hotspots (PHS) as villages that achieved less than 35% reduction in prevalence and/or less than 50% reduction in infection intensity after 4 years of either school-based or community-wide MDA, either annually or twice in 4 years. By this definition, at least 30% of villages in each of the five studies were PHSs. We found no consistent relationship between PHSs and the type or frequency of intervention, adequacy of reported MDA coverage, and prevalence or intensity of infection at baseline. New research is warranted to identify PHSs after just one or a few rounds of MDA, and new adaptive strategies need to be advanced and validated for turning PHSs into responder villages.
Figures
References
-
- World Health Organization , 2001. Fifty-Fourth World Health Assembly Resolution WHA54.19 Schistosomiasis and Soil-Transmitted Helminth Infections. Geneva, Switzerland: World Health Organization Fifty-Fourth World Health Assembly.
-
- World Health Organization , 2012. Sixty-Fifth World Health Assembly Resolution WHA65.21 Elimination of Schistosomiasis. Geneva, Switzerland: World Health Organization Sixty-Fifth World Health Assembly.
-
- World Health Organization , 2013. Sixty-Sixth World Health Assembly Resolution WHA66.12 Neglected Tropical Diseases. Geneva, Switzerland: World Health Organization Sixty-Sixth World Health Assembly.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
