

Strong muscles, weak heart: testosterone-induced cardiomyopathy
- PMID: 31287235
- PMCID: PMC6816072
- DOI: 10.1002/ehf2.12494
Strong muscles, weak heart: testosterone-induced cardiomyopathy
Abstract
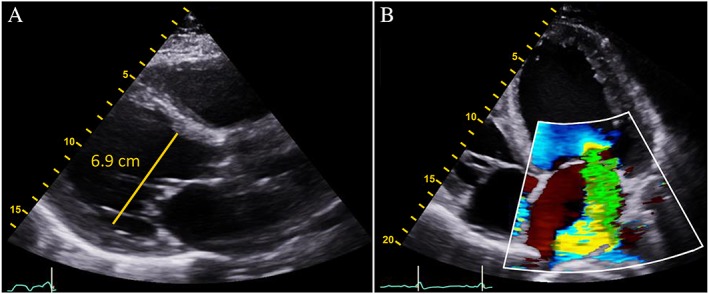
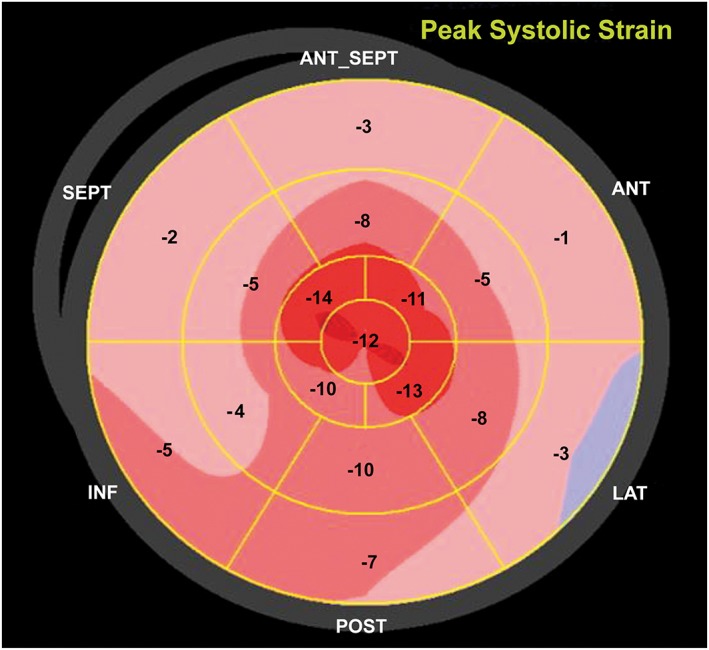
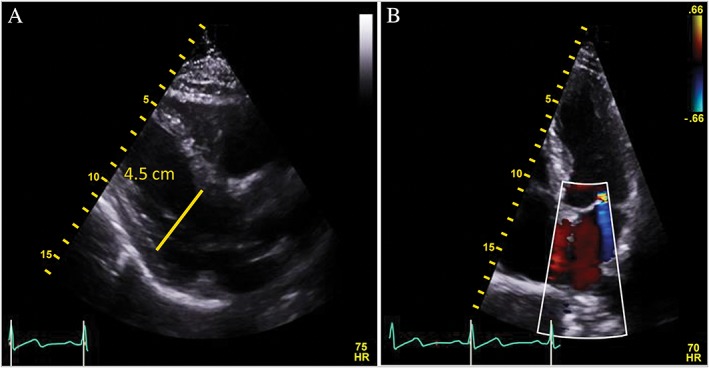
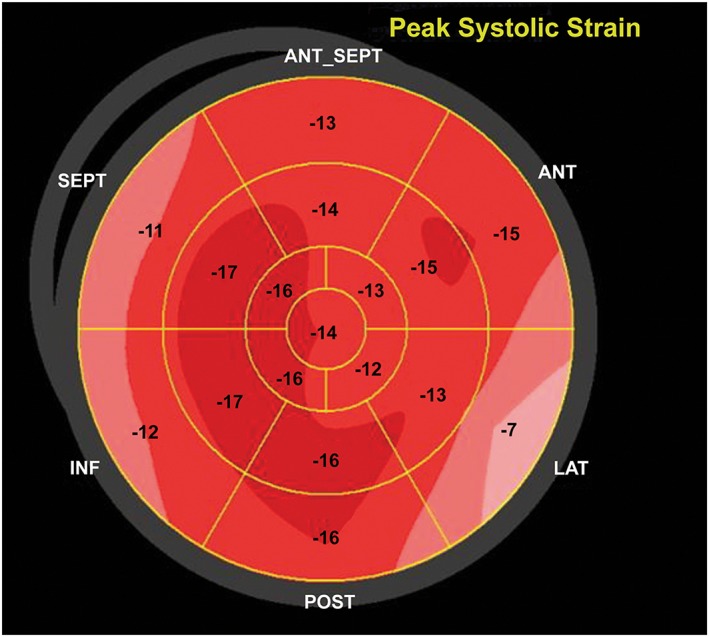
Exogenous anabolic androgen steroid use is associated with adverse cardiovascular outcomes. A 53-year-old bodybuilder presented with 3 months of exertional dyspnoea. Physical examination showed tachycardia and pan-systolic murmur; an echocardiogram showed a left ventricular ejection fraction (EF) of 15%. Evaluations included normal coronary angiogram, iron panel and thyroid studies, a negative viral panel (human immunodeficiency virus, Lyme disease, and hepatitis), and urine toxicology. He admitted to intramuscular anabolic steroid use; his testosterone level was 30 160.0 ng/dL (normal 280-1100 ng/dL). In addition to discontinuation of anabolic steroid use, he was treated with guideline-directed heart failure medical therapy. Repeat echocardiogram at 6 months showed an EF of 54% and normalized testosterone level of 603.7 ng/dL. Anabolic steroid use is a rare, reversible cause of cardiomyopathy in young, otherwise healthy athletes; a high index of suspicion is required to prevent potentially fatal side effects.
Keywords: Anabolic hormones; Cardiomyopathy; Testosterone.
© 2019 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Lichtenfeld J, Deal BJ, Crawford S. Sudden cardiac arrest following ventricular fibrillation attributed to anabolic steroid use in an adolescent. Cardiol Young 2016; 26: 996–998. - PubMed
-
- Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore longitudinal study of aging. J Clin Endocrinol Metab 2001; 86: 724–731. - PubMed
-
- Woolf PD, Hamill RW, McDonald JV, Lee LA, Kelly M. Transient hypogonadotropic hypogonadism caused by critical illness. J Clin Endocrinol Metab 1985; 60: 444–450. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
