

Patient, Neighborhood, and Spatial Determinants of Out-of-Hospital Cardiac Arrest Outcomes Throughout the Chain of Survival: A Community-Oriented Multilevel Analysis
- PMID: 31287347
- PMCID: PMC7000295
- DOI: 10.1080/10903127.2019.1640324
Patient, Neighborhood, and Spatial Determinants of Out-of-Hospital Cardiac Arrest Outcomes Throughout the Chain of Survival: A Community-Oriented Multilevel Analysis
Abstract
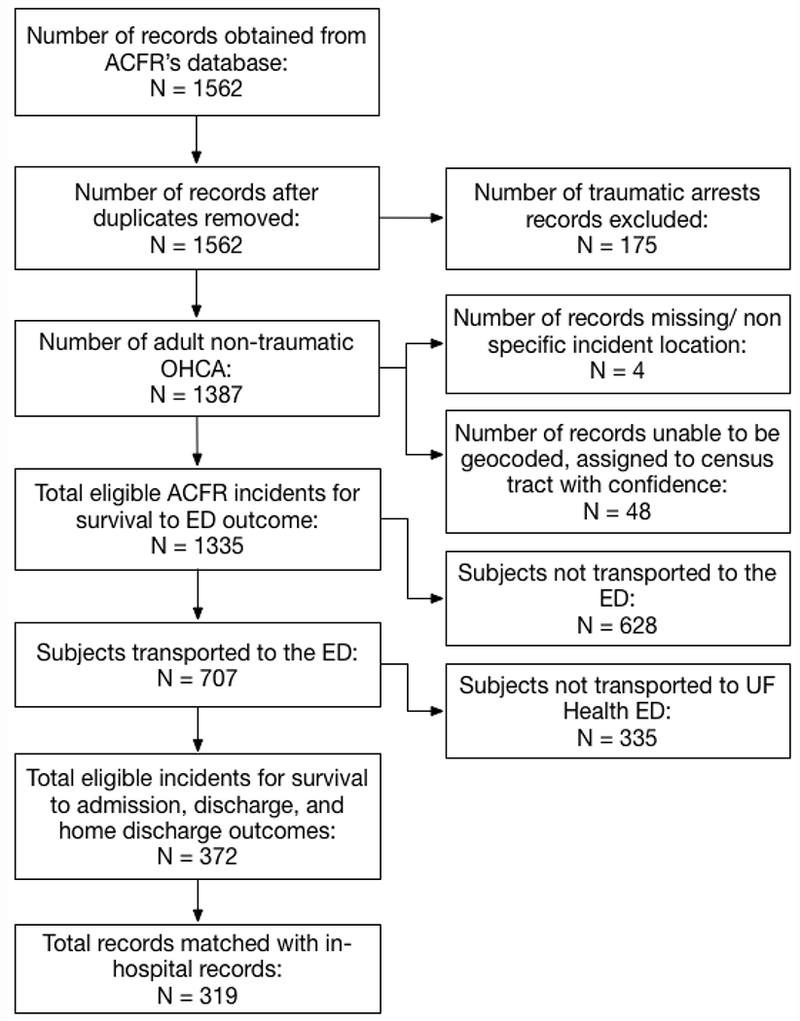
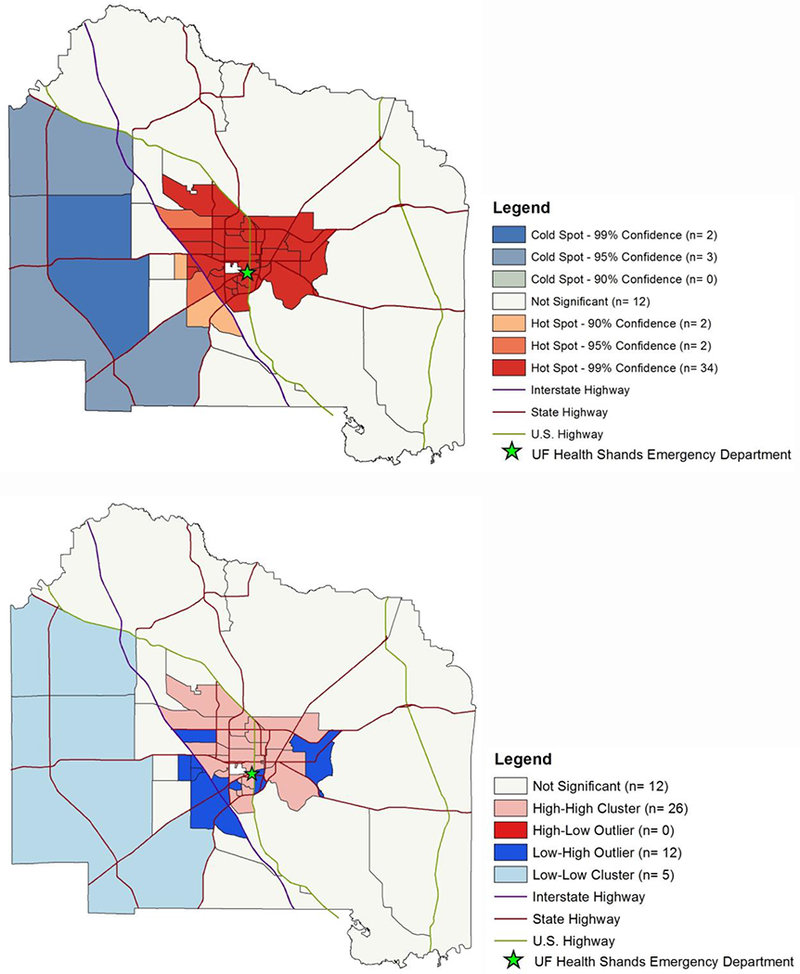
Objective: Global and national trends of out-of-hospital cardiac arrest (OHCA) have been examined; however, geographic variation and socioeconomic disparities of OHCA outcomes in the community setting are less understood. We developed and tested a replicable, community-oriented assessment strategy aimed to identify spatial variations in OHCA outcomes using socioeconomic, prehospital, and in-hospital factors. Methods: Emergency medical service (EMS) records of adult, non-traumatic OHCA within Alachua County, FL (2012-2017) were retrospectively reviewed and matched to corresponding medical records at the University of Florida (UF). Incidence of cardiac arrest was geocoded to census tracts and connected to U.S. census socioeconomic attribute data. Primary outcomes include survival to emergency department (ED), hospital admission, discharge, and discharge to home. Multilevel mixed-effects logistic regression models were developed to assess sub-county geographic variance, probabilities of survival, and prehospital risk factors. Getis-Ord Gi statistic and Moran's I-test was applied to assess spatial clustering in outcome survival rates. Results: Of the 1562 OHCA cases extracted from EMS records, 1,335 (85.5%) were included with 372 transported to study site. Predicted probability of survival to ED was 57.0% (95CI: 51.3-62.3%). Of transported cases to study site ED, predicted probabilities of survival was to 41.7% (95CI: 36.1-47.6%) for hospital admission, 16.1% (95CI: 10.7-23.5%) for hospital discharge, and 7.1% (95CI: 3.7-13.3%) for home discharge. Census tracts accounted for significant variability in survival to ED (p < 0.001), discharge (p = 0.031), and home discharge outcomes (p = 0.036). There was no significant geographic variation in survival to admission outcome. Neighborhood-level factors significantly improved model fit for survival to ED, discharge, and discharge home outcomes. Multiple modifiable patient- and neighborhood-level variables of interest were identified, including rural-urban differences. Conclusion: We identified important geographic disparities that exist in OHCA outcomes at the community level. By using a replicable schematic, this variation can be explained through community-oriented modifiable socioeconomic and prehospital factors.
Keywords: chain of survival; community-based; neurological outcomes; out-of-hospital cardiac arrest; prehospital; spatial distribution.
Conflict of interest statement
Conflict of Interests:
The authors report no conflict of interest
Figures

References
-
- Muller D, Agrawal R, Arntz HR. How sudden is sudden cardiac death? Circulation. 2006;114:1146–1150. - PubMed
-
- Cummins RO, Ornato JP, Thies WH, Pepe PE. Improving survival from sudden cardiac arrest: the “chain of survival” concept. A statement for health professionals from the Advanced Cardiac Life Support Subcommittee and the Emergency Cardiac Care Committee, American Heart Association. Circulation. 1991;83:1832–1847. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical