

Is knowledge of HIV status associated with sexual behaviours? A fixed effects analysis of a female sex worker cohort in urban Uganda
- PMID: 31287625
- PMCID: PMC6615530
- DOI: 10.1002/jia2.25336
Is knowledge of HIV status associated with sexual behaviours? A fixed effects analysis of a female sex worker cohort in urban Uganda
Abstract
Introduction: Female sex workers (FSWs) have strong economic incentives for sexual risk-taking behaviour. We test whether knowledge of HIV status affects such behaviours among FSWs.
Methods: We used longitudinal data from a FSW cohort in urban Uganda, which was formed as part of an HIV self-testing trial with four months of follow-up. Participants reported perceived knowledge of HIV status, number of clients per average working night, and consistent condom use with clients at baseline, one month, and four months. We measured the association between knowledge of HIV status and FSWs' sexual behaviours using linear panel regressions with individual fixed effects, controlling for study round and calendar time.
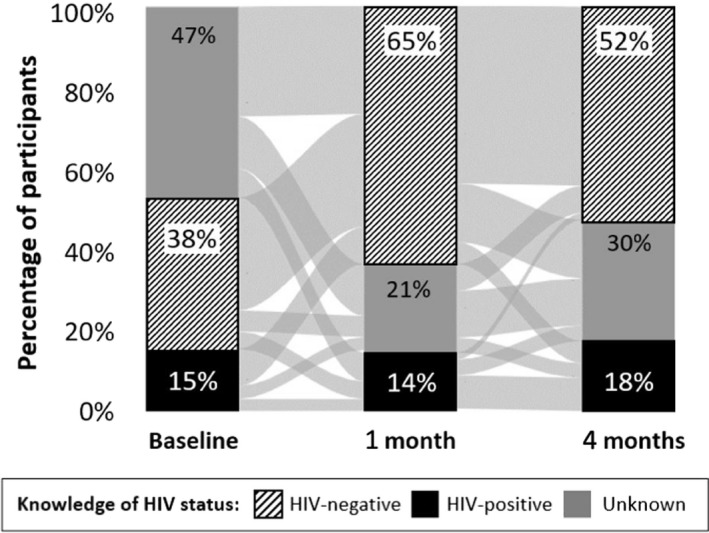
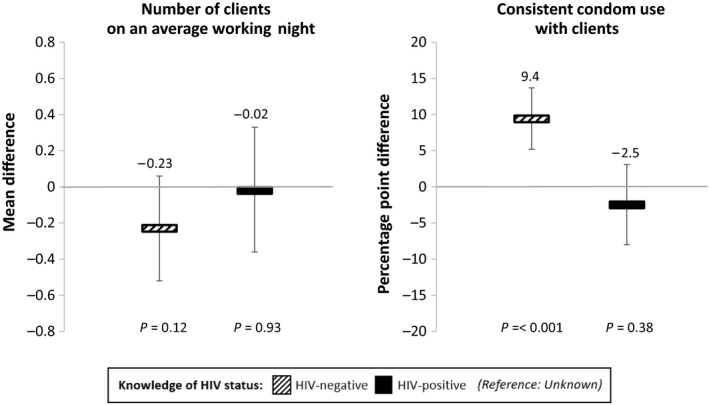
Results: Most of the 960 participants tested for HIV during the observation period (95%) and experienced a change in knowledge of HIV status (71%). Knowledge of HIV status did not affect participants' number of clients but did affect their consistent condom use. After controlling for individual fixed effects, study round and calendar month, knowledge of HIV-negative status was associated with a significant increase in consistent condom use by 9.5 percentage points (95% CI 5.2 to 13.5, p < 0.001), while knowledge of HIV-positive status was not associated with a significant change in consistent condom use (2.5 percentage points, 95% CI -8.0 to 3.1, p = 0.38).
Conclusions: In urban Uganda, FSWs engaged in safer sex with clients when they perceived that they themselves were not living with HIV. Even in communities with very high HIV prevalence, the majority of the population will test HIV-negative. Our results thus imply that expansion of HIV testing programmes may serve as a behavioural HIV prevention measure among FSWs.
Keywords: Knowledge of HIV status; Uganda; condom use; key and vulnerable populations; sex workers; sexual behaviours; testing; women.
© 2019 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Figures

Similar articles
-
Perceived Knowledge of HIV-Negative Status Increases Condom Use Among Female Sex Workers in Zambian Transit Towns.AIDS Patient Care STDS. 2020 Apr;34(4):184-192. doi: 10.1089/apc.2019.0266. AIDS Patient Care STDS. 2020. PMID: 32324483 Free PMC article.
-
Knowledge, attitudes & barriers to condom use among female sex workers and truck drivers in Uganda: a mixed-methods study.Afr Health Sci. 2013 Dec;13(4):1027-33. doi: 10.4314/ahs.v13i4.24. Afr Health Sci. 2013. PMID: 24940328 Free PMC article.
-
Relationship between reported prior condom use and current self-perceived risk of acquiring HIV among mobile female sex workers in southern India.BMC Public Health. 2011 Dec 29;11 Suppl 6(Suppl 6):S5. doi: 10.1186/1471-2458-11-S6-S5. BMC Public Health. 2011. PMID: 22375731 Free PMC article.
-
Are female sex workers able to negotiate condom use with male clients? The case of mobile FSWs in four high HIV prevalence states of India.PLoS One. 2013 Jun 28;8(6):e68043. doi: 10.1371/journal.pone.0068043. Print 2013. PLoS One. 2013. PMID: 23840806 Free PMC article.
-
A dose-response relationship between exposure to a large-scale HIV preventive intervention and consistent condom use with different sexual partners of female sex workers in southern India.BMC Public Health. 2011 Dec 29;11 Suppl 6(Suppl 6):S8. doi: 10.1186/1471-2458-11-S6-S8. BMC Public Health. 2011. PMID: 22375863 Free PMC article.
Cited by
-
Assessing young Kenyan women's willingness to engage in a peer-delivered HIV self-testing and referral model for PrEP initiation: A qualitative formative research study.Front Public Health. 2022 Oct 6;10:932948. doi: 10.3389/fpubh.2022.932948. eCollection 2022. Front Public Health. 2022. PMID: 36276357 Free PMC article.
-
Prevalence of Paid Sex and Associated Factors Among Women and Men Attending HIV Voluntary Counseling and Testing in Kinshasa, Democratic Republic of the Congo: A Prospective Cohort.Arch Sex Behav. 2024 Oct;53(9):3625-3637. doi: 10.1007/s10508-024-02939-w. Epub 2024 Aug 15. Arch Sex Behav. 2024. PMID: 39147958 Free PMC article.
-
The experiences of women from <em>Atoin Meto</em> tribe who performed <em>Sifon</em> ritual in the context of HIV/AIDS transmission.J Public Health Res. 2021 May 31;10(s1):jphr.2021.2337. doi: 10.4081/jphr.2021.2337. J Public Health Res. 2021. PMID: 34060742 Free PMC article.
-
Formalized peer referral to HIV pre-exposure prophylaxis supported with self-testing: a mixed-methods pilot study among young Kenyan women.Front Public Health. 2024 Sep 11;12:1428609. doi: 10.3389/fpubh.2024.1428609. eCollection 2024. Front Public Health. 2024. PMID: 39324163 Free PMC article.
-
Delivery of WeChat-Based HIV Result e-Reports in Social Networks for Recruitment of High-Risk Population: Baseline Data From a Cluster Randomized Controlled Trial.J Med Internet Res. 2023 Jun 15;25:e46793. doi: 10.2196/46793. J Med Internet Res. 2023. PMID: 37318850 Free PMC article. Clinical Trial.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
