

Endovascular Treatment: The Role of Dominant Caliber M2 Segment Occlusion in Ischemic Stroke
- PMID: 31287757
- PMCID: PMC6358188
- DOI: 10.1161/STROKEAHA.118.023117
Endovascular Treatment: The Role of Dominant Caliber M2 Segment Occlusion in Ischemic Stroke
Erratum in
-
Correction to: Endovascular Treatment: The Role of Dominant Caliber M2 Segment Occlusion in Ischemic Stroke.Stroke. 2019 Mar;50(3):e100. doi: 10.1161/STR.0000000000000185. Epub 2019 Feb 25. Stroke. 2019. PMID: 31287779 Free PMC article. No abstract available.
Abstract
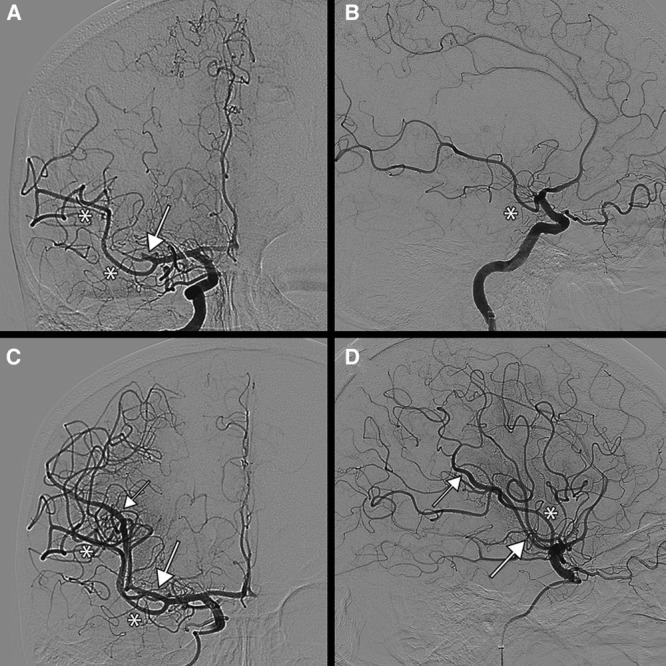
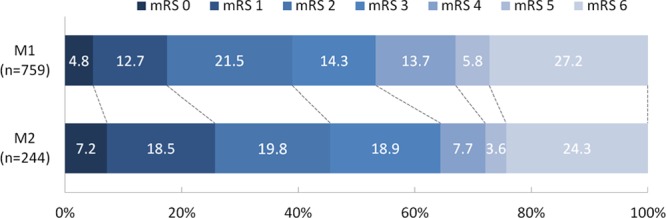
Background and Purpose- It is unclear whether endovascular treatment (EVT) is beneficial for patients with acute ischemic stroke with occlusion of the M2 segment of the middle cerebral artery. We aimed to compare functional outcomes, technical aspects, and complications of EVT between patients with acute ischemic stroke because of M2 and M1 occlusions in clinical practice. Furthermore, outcome and complications after EVT in dominant and nondominant caliber M2 division occlusions were studied. Methods- Data were obtained from the MR CLEAN Registry (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) which is an ongoing observational study in 16 Dutch centers performing EVT in the Netherlands. Functional outcome was measured with the modified Rankin Scale score at 90 days. Neurological recovery (delta National Institutes of Health Stroke Scale), successful reperfusion rates (extended Thrombolysis in Cerebral Infarction ≥2B), and safety outcomes were also investigated. Associations between occlusion location and outcome were analyzed with ordinal logistic regression models, with adjustment for other prognostic factors. Results- In total, 244 (24%) patients with an M2 and 759 (76%) patients with an M1 occlusion who underwent EVT were analyzed. Functional outcomes were not significantly different between patients with M2 versus M1 occlusions (adjusted common odds ratio, 1.24; 95% CI, 0.87-1.73). Occurrence of symptomatic intracerebral hemorrhage was also similar for M2 and M1 occlusions (6.6% versus 5.9%; P=0.84). Further analysis about dominance of an M2 branch was performed in 175 (72%) patients. Neurological recovery was comparable (mean delta National Institutes of Health Stroke Scale, -2±10 for dominant M2, -5±5 for nondominant M2, and -4±9 [ P=0.24] for M1 occlusions). Furthermore, the effect of reperfusion status on functional outcome was comparable between occlusion divisions (common odds ratio, 1.27; 95% CI, 1.06-1.53 for dominant M2; common odds ratio, 1.32; 95% CI, 0.93-1.87 for nondominant M2; and common odds ratio, 1.35; 95% CI, 1.24-1.46 for M1 occlusions). Conclusions- Outcomes and complication rates after EVT were similar in patients with M2 and M1 occlusions. Although based on observational data and a limited sample size, a similar association of reperfusion status with functional outcome for all subgroups provides no evidence that patients with either a dominant or a nondominant M2 occlusion should be routinely excluded from EVT.
Keywords: middle cerebral artery; reperfusion; stroke; thrombectomy; treatment outcome.
Figures
References
-
- Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. HERMES C; ollaborators. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387:1723–1731. doi: 10.1016/S0140-6736(16)00163-X. - PubMed
-
- Tomsick TA, Carrozzella J, Foster L, Hill MD, von Kummer R, Goyal M, et al. IMS III Investigators. Endovascular therapy of M2 occlusion in IMS III: role of M2 segment definition and location on clinical and revascularization outcomes. AJNR Am J Neuroradiol. 2017;38:84–89. doi: 10.3174/ajnr.A4979. - PMC - PubMed
-
- del Zoppo GJ, Poeck K, Pessin MS, Wolpert SM, Furlan AJ, Ferbert A, et al. Recombinant tissue plasminogen activator in acute thrombotic and embolic stroke. Ann Neurol. 1992;32:78–86. doi: 10.1002/ana.410320113. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
