

Pan-cancer Convergence to a Small-Cell Neuroendocrine Phenotype that Shares Susceptibilities with Hematological Malignancies
- PMID: 31287989
- PMCID: PMC6703903
- DOI: 10.1016/j.ccell.2019.06.005
Pan-cancer Convergence to a Small-Cell Neuroendocrine Phenotype that Shares Susceptibilities with Hematological Malignancies
Abstract
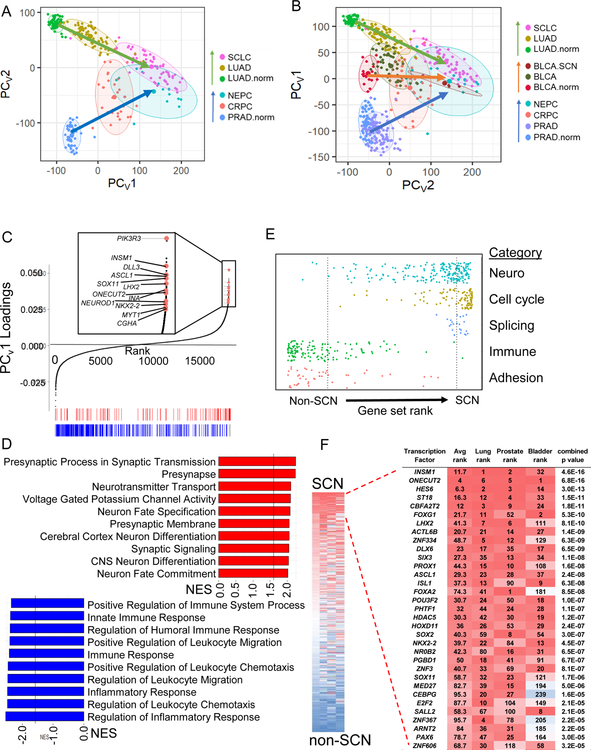
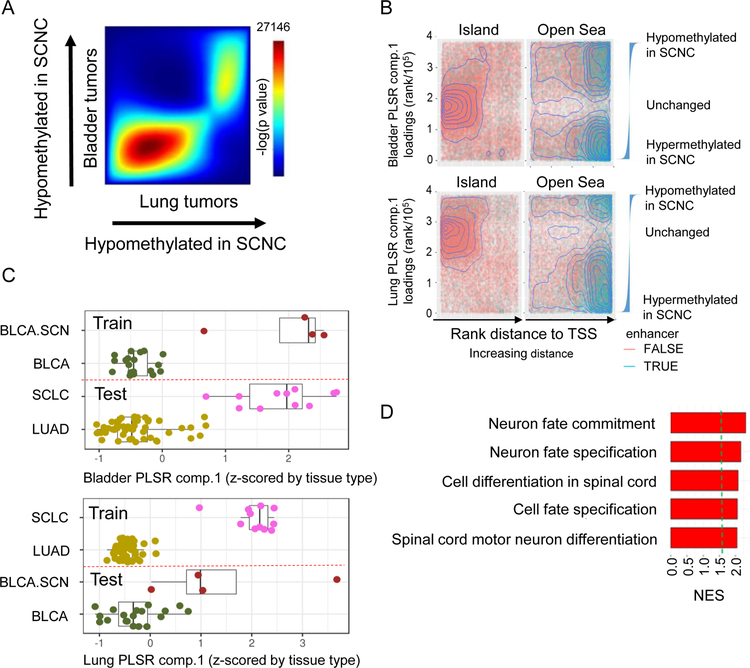
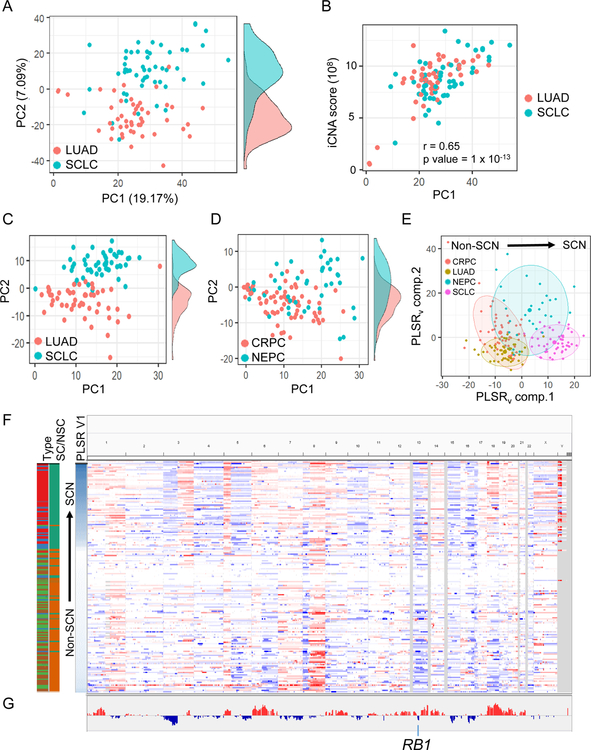
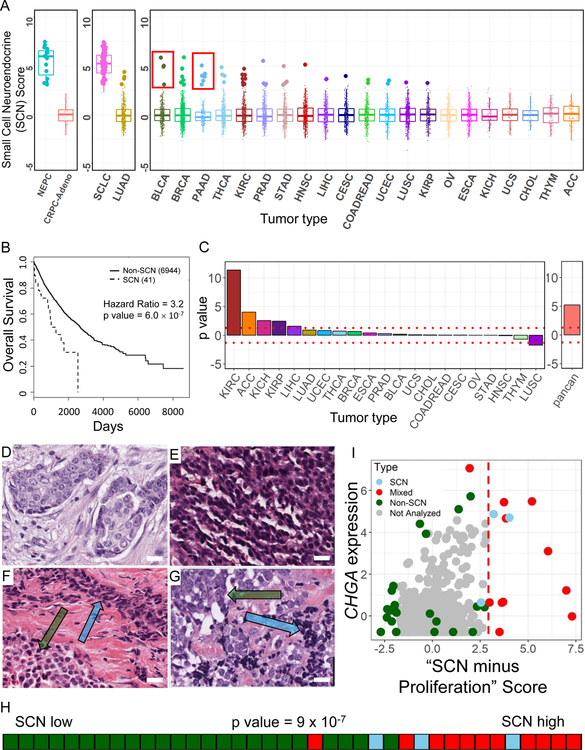
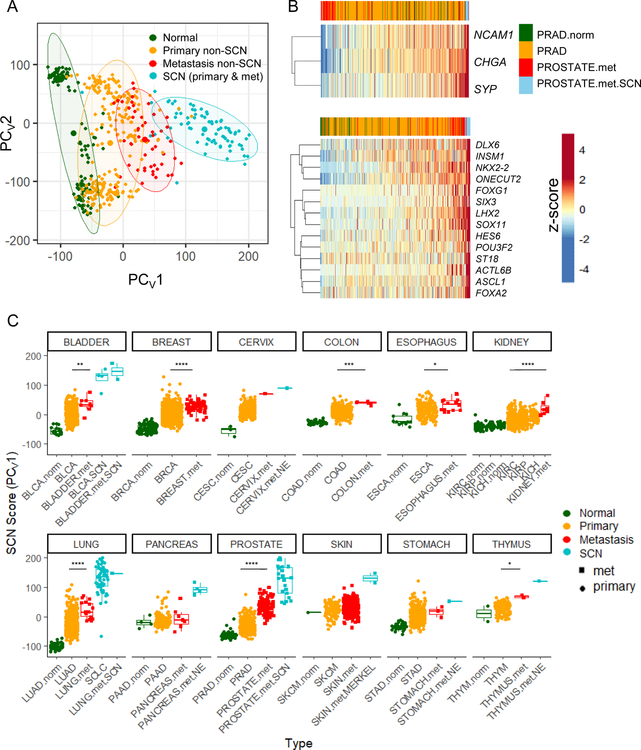
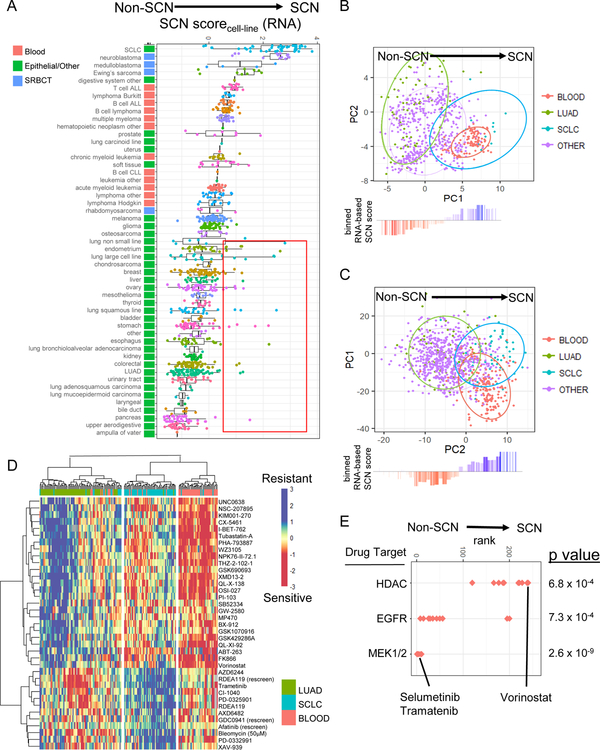
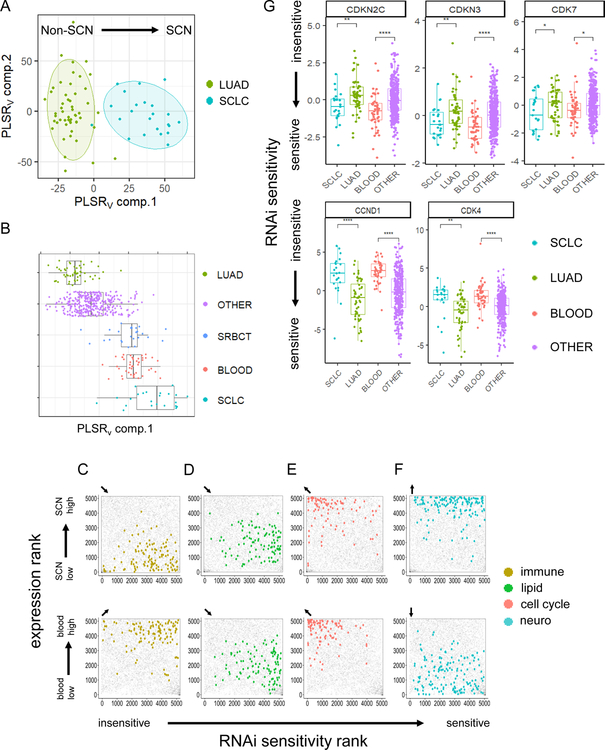
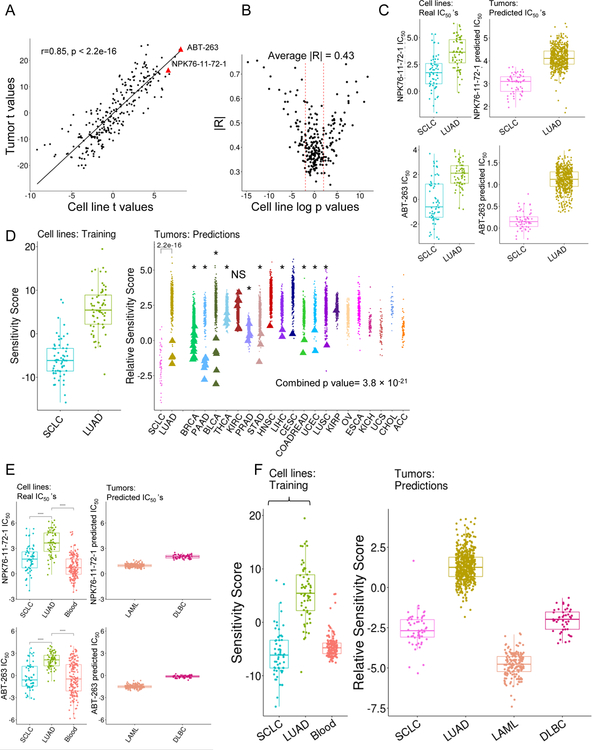
Small-cell neuroendocrine cancers (SCNCs) are an aggressive cancer subtype. Transdifferentiation toward an SCN phenotype has been reported as a resistance route in response to targeted therapies. Here, we identified a convergence to an SCN state that is widespread across epithelial cancers and is associated with poor prognosis. More broadly, non-SCN metastases have higher expression of SCN-associated transcription factors than non-SCN primary tumors. Drug sensitivity and gene dependency screens demonstrate that these convergent SCNCs have shared vulnerabilities. These common vulnerabilities are found across unannotated SCN-like epithelial cases, small-round-blue cell tumors, and unexpectedly in hematological malignancies. The SCN convergent phenotype and common sensitivity profiles with hematological cancers can guide treatment options beyond tissue-specific targeted therapies.
Keywords: Dependency Map (depmap); RNA interference screen; SCLC; TCGA; blood cancer; drug sensitivity screen; pan-cancer signatures; pharmacogenomics; small-cell neuroendocrine; transdifferentiation.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests
ONW currently has consulting, equity, and/or board relationships with Trethera Corporation, Kronos Biosciences, Sofie Biosciences, and Allogene Therapeutics. None of these companies contributed to or directed any of the research reported in this article.
Figures
Comment in
-
SCNC phenotypic convergence reveals shared vulnerabilities.Nat Rev Cancer. 2019 Oct;19(10):543. doi: 10.1038/s41568-019-0188-7. Nat Rev Cancer. 2019. PMID: 31371791 No abstract available.
References
-
- Alanee S, Moore A, Nutt M, Holland B, Dynda D, El-Zawahry A, and McVary KT (2015). Contemporary Incidence and Mortality Rates of Neuroendocrine Prostate Cancer. Anticancer Res 35, 4145–4150. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
