

Utility of Whole Blood Thiamine Pyrophosphate Evaluation in TPK1-Related Diseases
- PMID: 31288420
- PMCID: PMC6679130
- DOI: 10.3390/jcm8070991
Utility of Whole Blood Thiamine Pyrophosphate Evaluation in TPK1-Related Diseases
Abstract
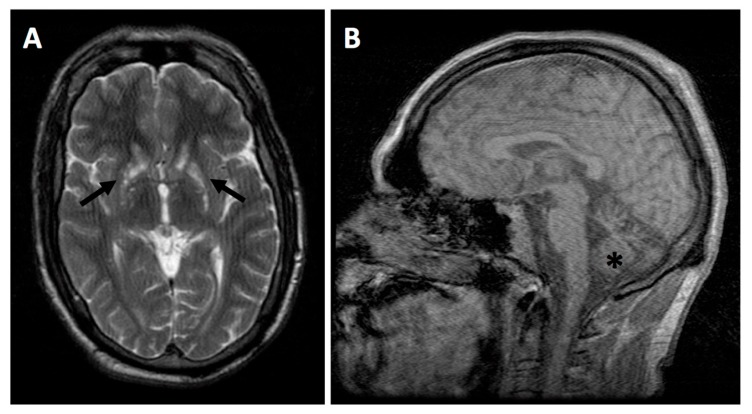
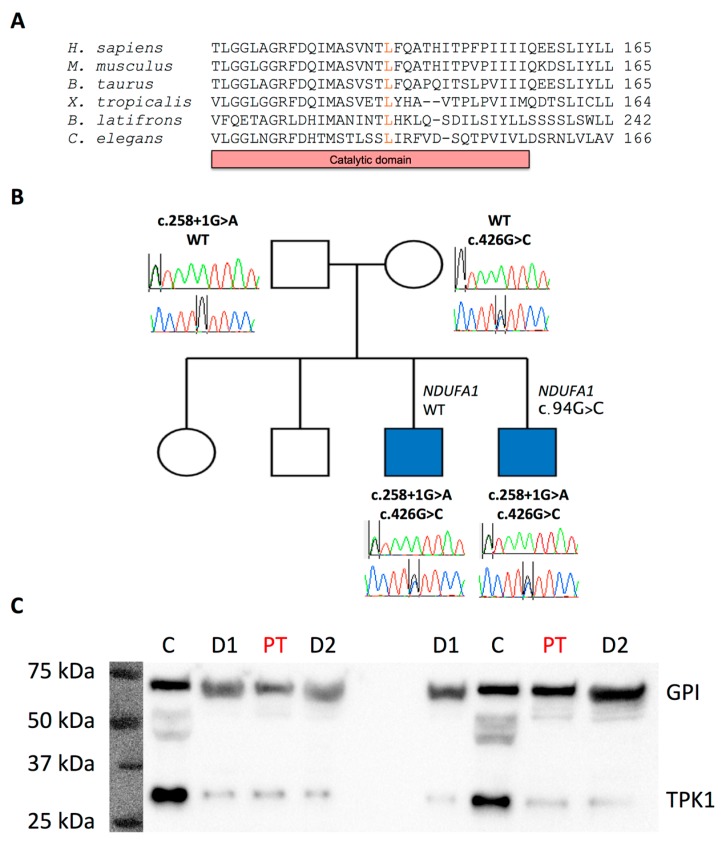
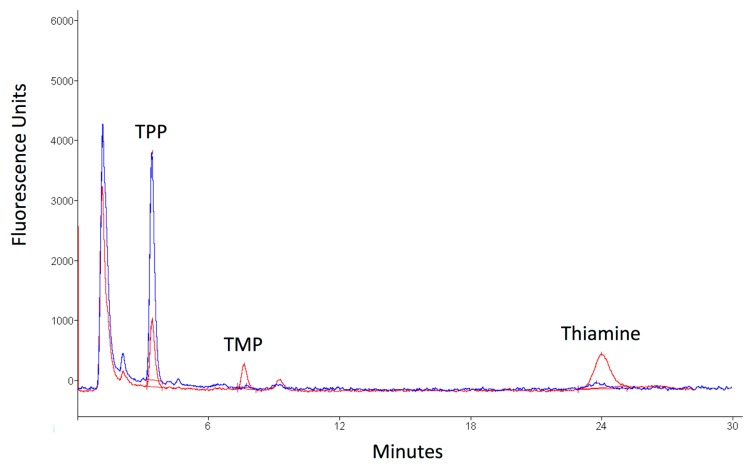
TPK1 mutations are a rare, but potentially treatable, cause of thiamine deficiency. Diagnosis is challenging given the phenotypic overlap that exists with other metabolic and neurological disorders. We report a case of TPK1-related disease presenting with Leigh-like syndrome and review the diagnostic utility of thiamine pyrophosphate (TPP) blood measurement. The proband, a 35-year-old male, presented at four months of age with recurrent episodes of post-infectious encephalopathy. He subsequently developed epilepsy, learning difficulties, sensorineural hearing loss, spasticity, and dysphagia. There was a positive family history for Leigh syndrome in an older brother. Plasma lactate was elevated (3.51 mmol/L) and brain MRI showed bilateral basal ganglia hyperintensities, indicative of Leigh syndrome. Histochemical and spectrophotometric analysis of mitochondrial respiratory chain complexes I, II+III, and IV was normal. Genetic analysis of muscle mitochondrial DNA was negative. Whole exome sequencing of the proband confirmed compound heterozygous variants in TPK1: c. 426G>C (p. Leu142Phe) and c. 258+1G>A (p.?). Blood TPP levels were reduced, providing functional evidence for the deleterious effects of the variants. We highlight the clinical and bioinformatics challenges to diagnosing rare genetic disorders and the continued utility of biochemical analyses, despite major advances in DNA sequencing technology, when investigating novel, potentially disease-causing, genetic variants. Blood TPP measurement represents a fast and cost-effective diagnostic tool in TPK1-related diseases.
Keywords: Leigh syndrome; TPK1; mitochondrial diseases; thiamine deficiency; thiamine pyrophosphate.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Potluri P., Davila A., Ruiz-Pesini E., Mishmar D., O’Hearn S., Hancock S., Simon M., Scheffler I.E., Wallace D.C., Procaccio V. A novel NDUFA1 mutation leads to a progressive mitochondrial complex I-specific neurodegenerative disease. Mol. Genet. Metab. 2009;96:189–195. doi: 10.1016/j.ymgme.2008.12.004. - DOI - PMC - PubMed
-
- Ortigoza-Escobar J.D., Alfadhel M., Molero-Luis M., Darin N., Spiegel R., de Coo I.F., Gerards M., Taylor R.W., Artuch R., Nashabat M., et al. Thiamine deficiency in childhood with attention to genetic causes: Survival and outcome predictors. Ann. Neurol. 2017;82:317–330. doi: 10.1002/ana.24998. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
