

Sociodemographic and geospatial associations with community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) infections in a large Canadian city: an 11 year retrospective study
- PMID: 31288765
- PMCID: PMC6617829
- DOI: 10.1186/s12889-019-7169-3
Sociodemographic and geospatial associations with community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) infections in a large Canadian city: an 11 year retrospective study
Abstract
Background: The first Canadian outbreak of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) was identified in 2004 in Calgary, Alberta. Using a novel model of MRSA population-based surveillance, sociodemographic risk associations, yearly geospatial dissemination and prevalence of CA-MRSA infections over an 11 year period was identified in an urban healthcare jurisdiction of Calgary.
Methods: Positive MRSA case records, patient demographics and laboratory data were obtained from a centralized Laboratory Information System of Calgary Laboratory Services in Calgary, Alberta, Canada between 2004 and 2014. Public census data was obtained from Statistics Canada, which was used to match with laboratory data and mapped using Geographic Information Systems.
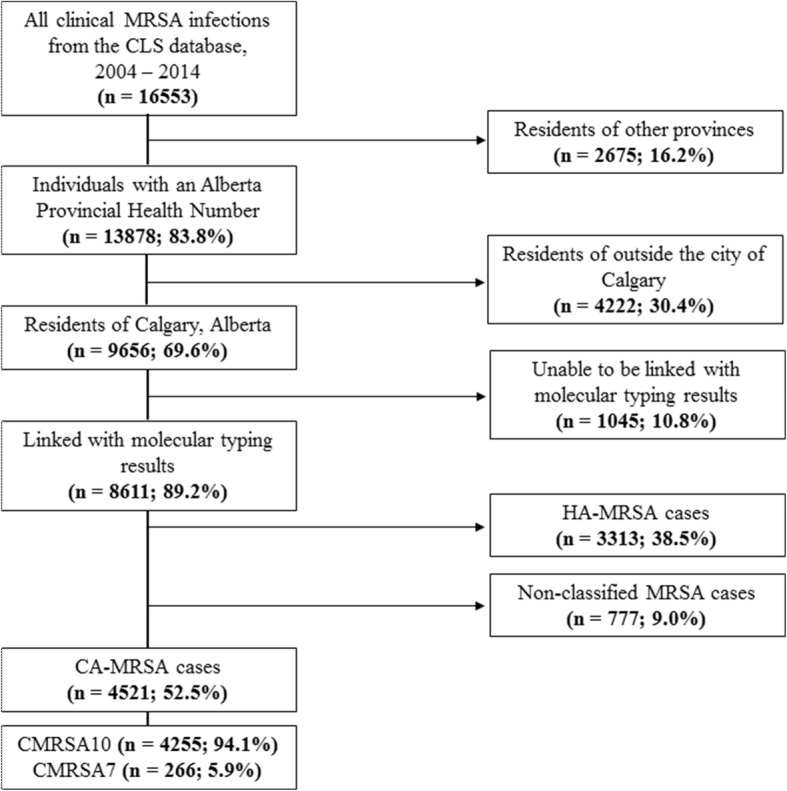
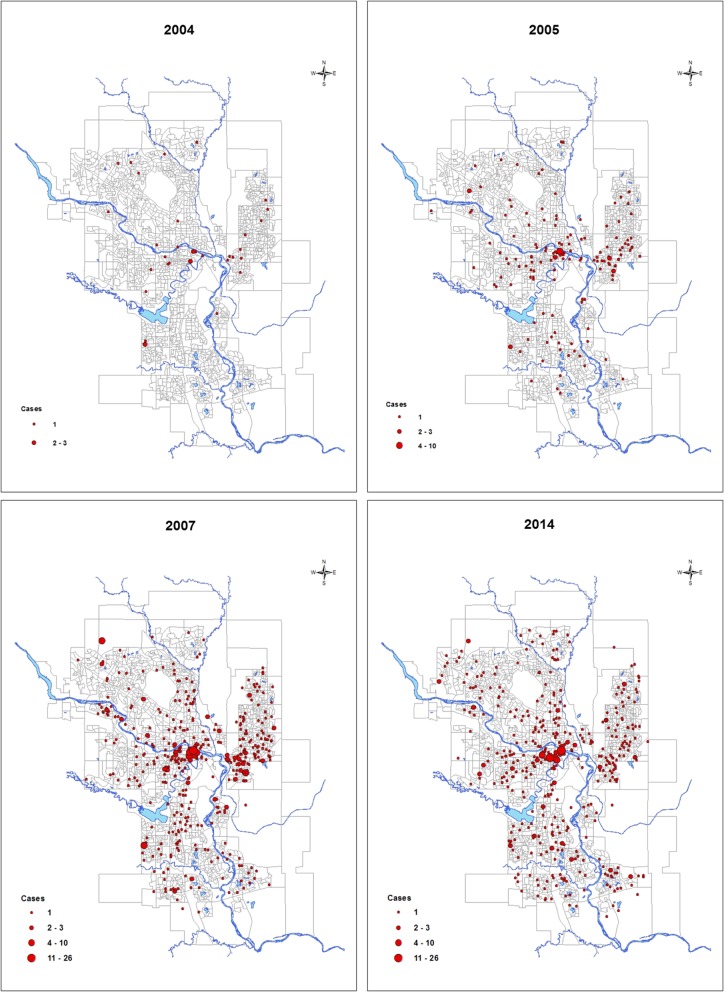
Results: During the study period, 52.5% of positive MRSA infections in Calgary were CA-MRSA cases. The majority were CMRSA10 (USA300) clones (94.1%; n = 4255), while the remaining case (n = 266) were CMRSA7 (USA400) clones. Period prevalence of CMRSA10 increased from 3.6 cases/100000 population in 2004, to 41.3 cases/100000 population in 2014. Geospatial analysis demonstrated wide dissemination of CMRSA10 annually in the city. Those who are English speaking (RR = 0.05, p < 0.0001), identify as visible minority Chinese (RR = 0.09, p = 0.0023) or visible minority South Asian (RR = 0.25, p = 0.015), and have a high median household income (RR = 0.27, p < 0.0001) have a significantly decreased relative risk of CMRSA10 infections.
Conclusions: CMRSA10 prevalence increased between 2004 and 2007, followed by a stabilization of cases by 2014. Certain sociodemographic factors were protective from CMRSA10 infections. The model of MRSA population-surveillance and geomap outbreak events can be used to track the epidemiology of MRSA in any jurisdiction.
Keywords: CA-MRSA; CMRSA10; Geospatial analysis; Laboratory medicine.
Conflict of interest statement
The authors declare they have no competing interests.
Figures
Similar articles
-
Comparing the epidemiology of hospital-acquired methicillin-resistant Staphylococcus aureus clone groups in Alberta, Canada.Epidemiol Infect. 2016 Jul;144(10):2184-90. doi: 10.1017/S0950268816000376. Epub 2016 Mar 7. Epidemiol Infect. 2016. PMID: 26947456 Free PMC article.
-
Emergence of new CMRSA7/USA400 methicillin-resistant Staphylococcus aureus spa types in Alberta, Canada, from 2005 to 2012.J Clin Microbiol. 2014 Jul;52(7):2439-46. doi: 10.1128/JCM.00505-14. Epub 2014 Apr 30. J Clin Microbiol. 2014. PMID: 24789179 Free PMC article.
-
Changing epidemiology of methicillin-resistant Staphylococcus aureus in Alberta, Canada: population-based surveillance, 2005-2008.Epidemiol Infect. 2011 Jul;139(7):1009-18. doi: 10.1017/S0950268810002128. Epub 2010 Sep 21. Epidemiol Infect. 2011. PMID: 20854711
-
Global epidemiology of community-associated methicillin resistant Staphylococcus aureus (CA-MRSA).Curr Opin Microbiol. 2012 Oct;15(5):588-95. doi: 10.1016/j.mib.2012.08.003. Epub 2012 Oct 5. Curr Opin Microbiol. 2012. PMID: 23044073 Review.
-
Staphylococcus aureus: a community pathogen.Infect Dis Clin North Am. 2009 Mar;23(1):35-52. doi: 10.1016/j.idc.2008.10.002. Infect Dis Clin North Am. 2009. PMID: 19135915 Review.
Cited by
-
Genomic analysis of group A Streptococcus isolated during a correctional facility outbreak of MRSA in 2004.J Assoc Med Microbiol Infect Dis Can. 2022 Feb 24;7(1):23-35. doi: 10.3138/jammi-2021-0018. eCollection 2022 Mar. J Assoc Med Microbiol Infect Dis Can. 2022. PMID: 36340844 Free PMC article.
-
The association between socioeconomic factors and the success of decolonization treatment among individuals diagnosed with methicillin-resistant Staphylococcus aureus: A cohort study from 2007 to 2020.Infect Control Hosp Epidemiol. 2023 Oct;44(10):1620-1628. doi: 10.1017/ice.2023.32. Epub 2023 Apr 5. Infect Control Hosp Epidemiol. 2023. PMID: 37017132 Free PMC article.
-
Risk Factors and Outcomes of Bloodstream Infections Among People With Human Immunodeficiency Virus: A Longitudinal Cohort Study From 2000 to 2017.Open Forum Infect Dis. 2022 Aug 3;9(8):ofac318. doi: 10.1093/ofid/ofac318. eCollection 2022 Aug. Open Forum Infect Dis. 2022. PMID: 35937645 Free PMC article.
-
Bioguided Isolation of Active Compounds from Rhamnus alaternus against Methicillin-Resistant Staphylococcus aureus (MRSA) and Panton-Valentine Leucocidin Positive Strains (MSSA-PVL).Molecules. 2021 Jul 19;26(14):4352. doi: 10.3390/molecules26144352. Molecules. 2021. PMID: 34299627 Free PMC article.
-
Staphylococcus aureus in Agriculture: Lessons in Evolution from a Multispecies Pathogen.Clin Microbiol Rev. 2021 Feb 10;34(2):e00182-20. doi: 10.1128/CMR.00182-20. Print 2021 Mar 17. Clin Microbiol Rev. 2021. PMID: 33568553 Free PMC article. Review.
References
-
- King MD, Humphrey BJ, Wang YF, Kourbatova EV, Ray SM, Blumberg HM. Emergence of community-acquired methicillin-resistant Staphylococcus aureus USA 300 clone as the predominant cause of skin and soft-tissue infections. Ann Intern Med. 2006;144:309–317. doi: 10.7326/0003-4819-144-5-200603070-00005. - DOI - PubMed
-
- Gilbert M, MacDonald J, Gregson D, Siushansian J, Zhang K, Elsayed S, et al. Outbreak in Alberta of community-acquired (USA300) methicillin-resistant Staphylococcus aureus in people with a history of drug use, homelessness or incarceration. CMAJ. 2006;175:149–154. doi: 10.1503/cmaj.051565. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
