

Retroposed copies of RET gene: a somatically acquired event in medullary thyroid carcinoma
- PMID: 31288802
- PMCID: PMC6617568
- DOI: 10.1186/s12920-019-0552-1
Retroposed copies of RET gene: a somatically acquired event in medullary thyroid carcinoma
Abstract
Background: Different pathogenic germline mutations in the RET oncogene are identified in MEN 2, a hereditary syndrome characterized by medullary thyroid carcinoma (MTC) and other endocrine tumors. Although genetic predisposition is recognized, not all RET mutation carriers will develop the disease during their lifetime or, likewise, RET mutation carriers belonging to the same family may present clinical heterogeneity. It has been suggested that a single germline mutation might not be sufficient for development of MEN 2-associated tumors and a somatic bi-allelic alteration might be required. Here we investigated the presence of somatic second hit mutation in the RET gene in MTC.
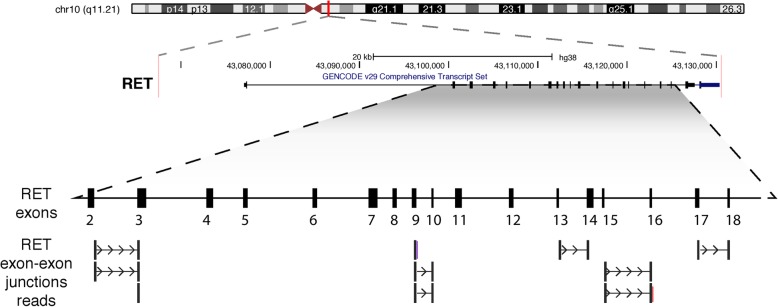
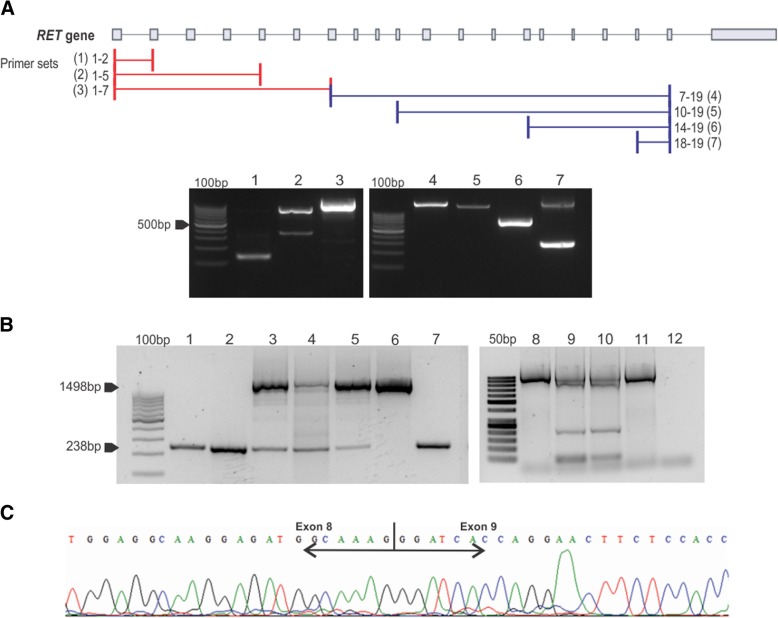
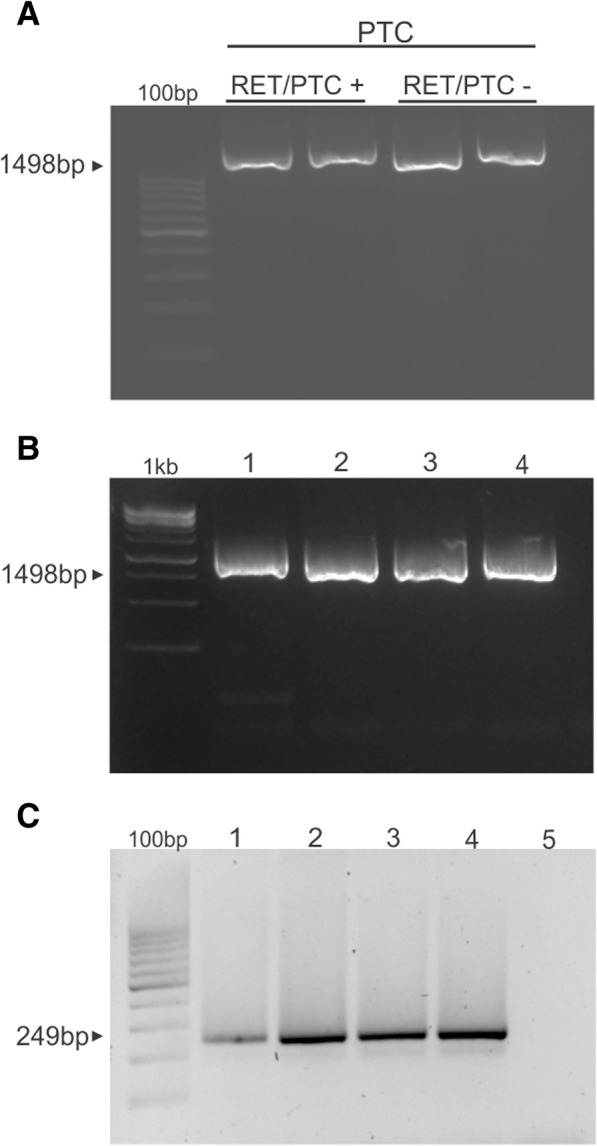
Methods: We integrated Multiplex Ligation-dependent Probe Amplification (MLPA) and whole exome sequencing (WES) to search for copy number alteration (CNA) in the RET gene in MTC samples and medullary thyroid cell lines (TT and MZ-CR-1). We next found reads spanning exon-exon boundaries on RET, an indicative of retrocopy. We subsequently searched for RET retrocopies in the human reference genome (GRCh37) and in the 1000 Genomes Project data, by looking for reads reporting joined exons in the RET locus or distinct genomic regions. To determine RET retrocopy specificity and recurrence, DNA isolated from sporadic and MEN 2-associated MTC (n = 37), peripheral blood (n = 3) and papillary thyroid carcinomas with RET fusion (n = 10) samples were tested using PCR-sequencing methodology.
Results: Through MLPA we have found evidence of CNA in the RET gene in MTC samples and MTC cell lines. WES analysis reinforced the presence of the CNA and hinted for a retroposed copy of RET not found in the human reference genome and 1.000 Genomes Project. Extended analysis confirmed the presence of a somatic MTC-related retrocopy of RET in both sporadic and hereditary tumors. We further unveiled a recurrent (28%) novel point mutation (p.G548 V) found exclusively in the retrocopy of RET. The mutation was also found in cDNA of mutated samples, suggesting it might be functional.
Conclusion: We here report a somatic specific RET retroposed copy in MTC samples and cell lines. Our results support the idea that generation of retrocopies in somatic cells is likely to contribute to MTC genesis and progression.
Keywords: G548V; MEN 2; MTC; Medullary thyroid carcinoma; RET; Retrocopy; Second hit.
Conflict of interest statement
The authors reported no conflicts of interest.
Figures


References
-
- Eng C, Clayton D, Schuffenecker I, Lenoir G, Cote G, Gagel RF, van Amstel HK, Lips CJ, Nishisho I, Takai SI, et al. The relationship between specific RET proto-oncogene mutations and disease phenotype in multiple endocrine neoplasia type 2. International RET mutation consortium analysis. JAMA : the journal of the American Medical Association. 1996;276:1575–1579. doi: 10.1001/jama.1996.03540190047028. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
