

Assessment of the impact of availability and readiness of malaria services on uptake of intermittent preventive treatment in pregnancy (IPTp) provided during ANC visits in Tanzania
- PMID: 31288835
- PMCID: PMC6617666
- DOI: 10.1186/s12936-019-2862-3
Assessment of the impact of availability and readiness of malaria services on uptake of intermittent preventive treatment in pregnancy (IPTp) provided during ANC visits in Tanzania
Abstract
Background: Intermittent preventive treatment during pregnancy (IPTp) is a highly-recommended intervention to prevent maternal and neonatal complications associated with malaria infection. Despite fairly high antenatal care (ANC) coverage in Tanzania, low IPTp uptake rates represent a gap in efforts to decrease complications attributed to malaria in pregnancy. The objective of this study was to examine if availability, readiness and managing authority are associated with uptake of IPTp during ANC.
Methods: Data for this analysis come from a cross-sectional survey, the Tanzania Service Provision Assessment conducted between 2014 and 2015. Principal component analysis was used to create scores for availability of malaria services and readiness for the provision of services. Generalized estimating equation models with logit link and the binomial distribution assessed factors that impact the uptake of IPTp by pregnant women attending ANC.
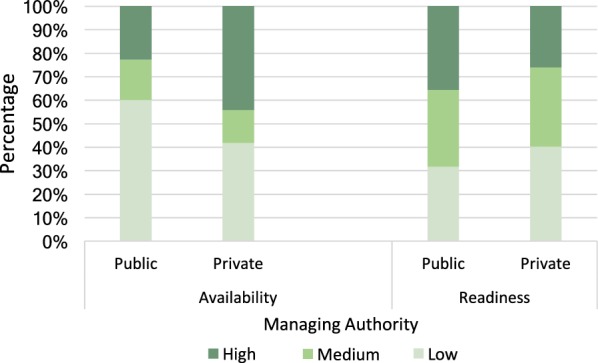
Results: Higher fraction of women in their third trimester than second (68% versus 49%, OR = 2.6; 95% CI (2.1-3.3)), had received at least one dose of IPTp. There was a wide variation in the availability and readiness of malaria services provision and diagnostic tools by managing authorities. Public facilities were more likely than private to offer malaria rapid diagnostic test, and more providers at public facilities than private diagnosed and/or treated malaria. Women who attended facilities where direct observation therapy was practiced were more likely to have received at least one dose of IPTp (64% versus 46% who received none; p < 0.001). Women who attended ANC at a facility with a high readiness score were more likely to take IPTp than those attending facilities with low readiness scores (OR = 2.1; 95% CI (1.4-3.3)). Reported stock out on the day of interview was negatively associated with IPTp uptake (OR 0.09; 95% CI 0.07-0.1).
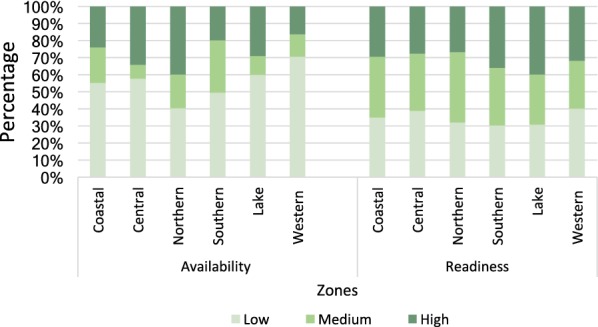
Conclusion: Readiness of health facilities to provide malaria related services, the number of ANC visits and gestational age were associated with uptake of IPTp among women attending ANC. There are disparities in malaria service availability and readiness across geographical location and managing authorities. These findings could be used to assist the malaria programme and policymakers to appropriately decide when planning for malaria service deliveries and interventions.
Keywords: Health services; IPTp; Malaria; Service availability; Service readiness; Tanzania.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The readiness of malaria services and uptake of intermittent preventive treatment in pregnancy in six sub-Saharan countries.J Glob Health. 2024 Jun 28;14:04112. doi: 10.7189/jogh.14.04112. J Glob Health. 2024. PMID: 38939971 Free PMC article.
-
Predictors for the uptake of optimal doses of sulfadoxine-pyrimethamine for intermittent preventive treatment of malaria during pregnancy in Tanzania: further analysis of the data of the 2015-2016 Tanzania demographic and health survey and malaria indicator survey.Malar J. 2021 Feb 6;20(1):75. doi: 10.1186/s12936-021-03616-2. Malar J. 2021. PMID: 33549094 Free PMC article.
-
Factors affecting uptake of ≥ 3 doses of Sulfadoxine-Pyrimethamine for malaria prevention in pregnancy in selected health facilities, Arusha region, Tanzania.BMC Pregnancy Childbirth. 2019 Nov 27;19(1):440. doi: 10.1186/s12884-019-2592-0. BMC Pregnancy Childbirth. 2019. PMID: 31775686 Free PMC article.
-
Determinants of uptake of intermittent preventive treatment during pregnancy: a review.Malar J. 2019 Nov 21;18(1):372. doi: 10.1186/s12936-019-3004-7. Malar J. 2019. PMID: 31752868 Free PMC article. Review.
-
Status of malaria in pregnancy services in Madagascar 2010-2021: a scoping review.Malar J. 2023 Feb 20;22(1):59. doi: 10.1186/s12936-023-04497-3. Malar J. 2023. PMID: 36803987 Free PMC article.
Cited by
-
Supply-side readiness to deliver HIV testing and treatment services in Indonesia: Going the last mile to eliminate mother-to-child transmission of HIV.PLOS Glob Public Health. 2022 Aug 3;2(8):e0000845. doi: 10.1371/journal.pgph.0000845. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962570 Free PMC article.
-
Experiences of young mothers with the uptake of Sulfadoxine-Pyrimethamine for intermittent preventive treatment of malaria in pregnancy: a cross-sectional study in the Lake endemic region, Kenya.Front Glob Womens Health. 2024 Mar 26;5:1294893. doi: 10.3389/fgwh.2024.1294893. eCollection 2024. Front Glob Womens Health. 2024. PMID: 38596532 Free PMC article.
-
Prevalence and Health System Determinants Of Uptake Of Three Or More Doses Of Sulphadoxine Pyrimethamine For Intermittent Preventive Treatment Of Malaria During Pregnancy.East Afr Med J. 2025 Jan 10;101(11):7552-7562. East Afr Med J. 2025. PMID: 40276557 Free PMC article.
-
The readiness of malaria services and uptake of intermittent preventive treatment in pregnancy in six sub-Saharan countries.J Glob Health. 2024 Jun 28;14:04112. doi: 10.7189/jogh.14.04112. J Glob Health. 2024. PMID: 38939971 Free PMC article.
-
Were Women Staying on Track with Intermittent Preventive Treatment for Malaria in Antenatal Care Settings? A Cross-Sectional Study in Senegal.Int J Environ Res Public Health. 2022 Oct 8;19(19):12866. doi: 10.3390/ijerph191912866. Int J Environ Res Public Health. 2022. PMID: 36232166 Free PMC article.
References
-
- Jhpiego. Prevention and Control of Malaria in pregnancy: reference manual. 3rd ed. Baltimore. 2018. http://resources.jhpiego.org/system/files/resources/01_MIPReferenceManua.... Accessed 15 Sept 2018.
-
- UNICEF. Low birthweight: country, regional and global estimates. 2004. https://www.unicef.org/publications/files/low_birthweight_from_EY.pdf. Accessed 25 Aug 2018.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
