

The Interdisciplinary Management of Foot Drop
- PMID: 31288916
- PMCID: PMC6637663
- DOI: 10.3238/arztebl.2019.0347
The Interdisciplinary Management of Foot Drop
Abstract
Background: Foot drop can be caused by a variety of diseases and injuries. Although it is a common condition, its overall incidence has not been reported to date. Foot drop markedly restricts the everyday activities of persons suffering from it. There is, therefore, a need for an optimized strategy for its diagnosis and treatment that would be standardized across the medical specialties encountering patients with this problem.
Methods: This article consists of a review on the basis of pertinent publications re- trieved by a search in the Pubmed/MEDLINE and Cochrane databases, as well as a description of the authors' proposed strategy for the diagnosis and treatment of foot drop.
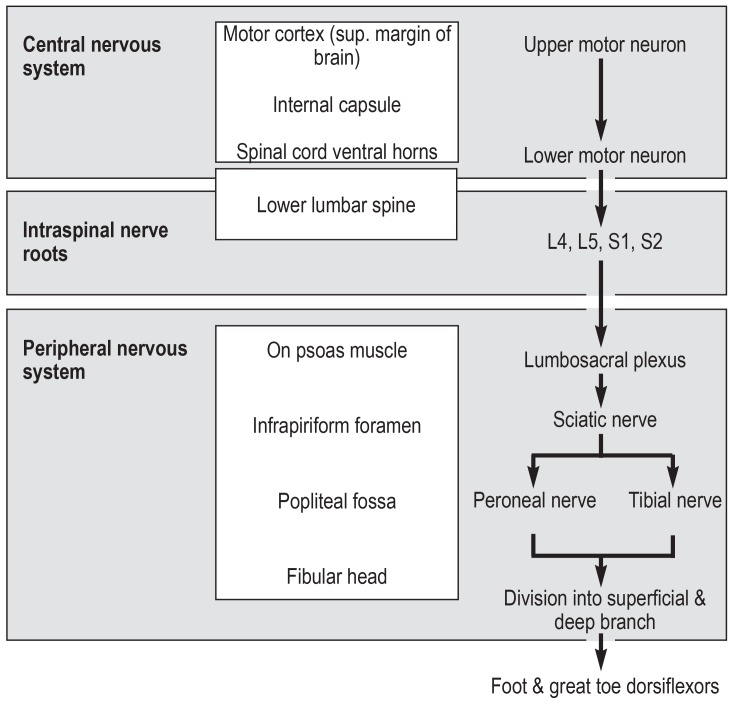
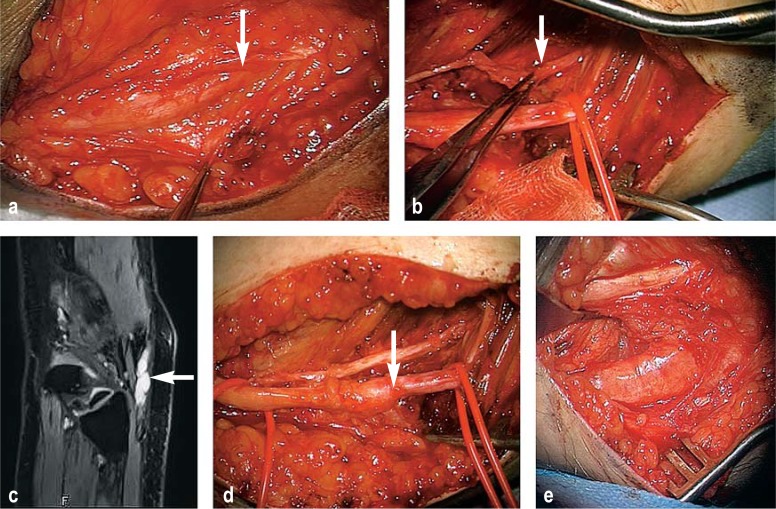
Results: Foot drop can be due to a disturbance at any central or peripheral location along the motor neural pathway that terminates in the dorsiflexor muscles of the foot, or at multiple locations in series. Optimal localization of the lesion(s) is a pre- requisite for appropriate treatment and a successful outcome. The most common causes are L5 radiculopathy and peroneal nerve injury. An operation by a neuro- surgeon or spinal surgeon is a reasonable option whenever there is a realistic chance that the nerve will recover. In our opinion, any patient with a subjectively disturbing foot drop and a clinically suspected compressive neuropathy of the peroneal nerve should be informed about the option of surgical decompression of the nerve at the fibular head, which can be performed with little risk. In case of a permanent foot drop, some patients can benefit from muscle-transfer surgery. For spastic foot drop, the option of botulinum toxin injections should be evaluated.
Conclusion: The care of patients with foot drop could be optimized by interdisciplin- ary foot-drop clinics involving all of the relevant specialists. The goals of treatment should always be improved mobility in everyday life and the prevention of falls, pain, and abnormal postures.
Figures


Comment in
-
Neuromuscular Electrical Stimulation (NMES) and α-Lipoic Acid.Dtsch Arztebl Int. 2019 Sep 20;116(38):643. doi: 10.3238/arztebl.2019.0643a. Dtsch Arztebl Int. 2019. PMID: 31617487 Free PMC article. No abstract available.
-
Anatomy Not Precisely Described.Dtsch Arztebl Int. 2019 Sep 20;116(38):643. doi: 10.3238/arztebl.2019.0643b. Dtsch Arztebl Int. 2019. PMID: 31617488 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2019 Sep 20;116\\Server1\dgi_work\Aerzteblatt\2019\10_SCH_CALE\Dtsch_Arztebl_Int-116_33-34\(38):643-644. doi: 10.3238/arztebl.2019.0643c. Dtsch Arztebl Int. 2019. PMID: 31617489 Free PMC article. No abstract available.
References
-
- Ewerbeck V, Wentzensen V, Holz F, Krämer KW, Pfeil J, Sabo D. Standardverfahren in der operativen Orthopädie und Unfallchirurgie. Thieme. (3) 2006
-
- Vlahovic TC, Ribeiro CE, Lamm BM, et al. A case of peroneal neuropathy-induced footdrop Correlated and compensatory lower-extremity function. Am Podiatr Med Assoc. 2000;90:411–420. - PubMed
-
- Aprile I, Caliandro P, La Torre G, et al. Multicenter study of peroneal mononeuropathy: clinical, neurophysiologic, and quality of life assessment. J Peripher Nerv Syst. 2005;10:259–268. - PubMed
-
- Upton AR, McComas AJ. The double crush in nerve entrapment syndromes. Lancet. 1973;2:359–362. - PubMed
-
- Matsumoto J, Isu T, Kim K, et al. Impact of additional treatment of paralumbar spine and peripheral nerve diseases after lumbar spine surgery. World Neurosurg. 2018;112:e778–e782. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical