

Immunologic Correlates of Pathologic Complete Response to Preoperative Immunotherapy in Hepatocellular Carcinoma
- PMID: 31289040
- PMCID: PMC7726707
- DOI: 10.1158/2326-6066.CIR-18-0605
Immunologic Correlates of Pathologic Complete Response to Preoperative Immunotherapy in Hepatocellular Carcinoma
Abstract
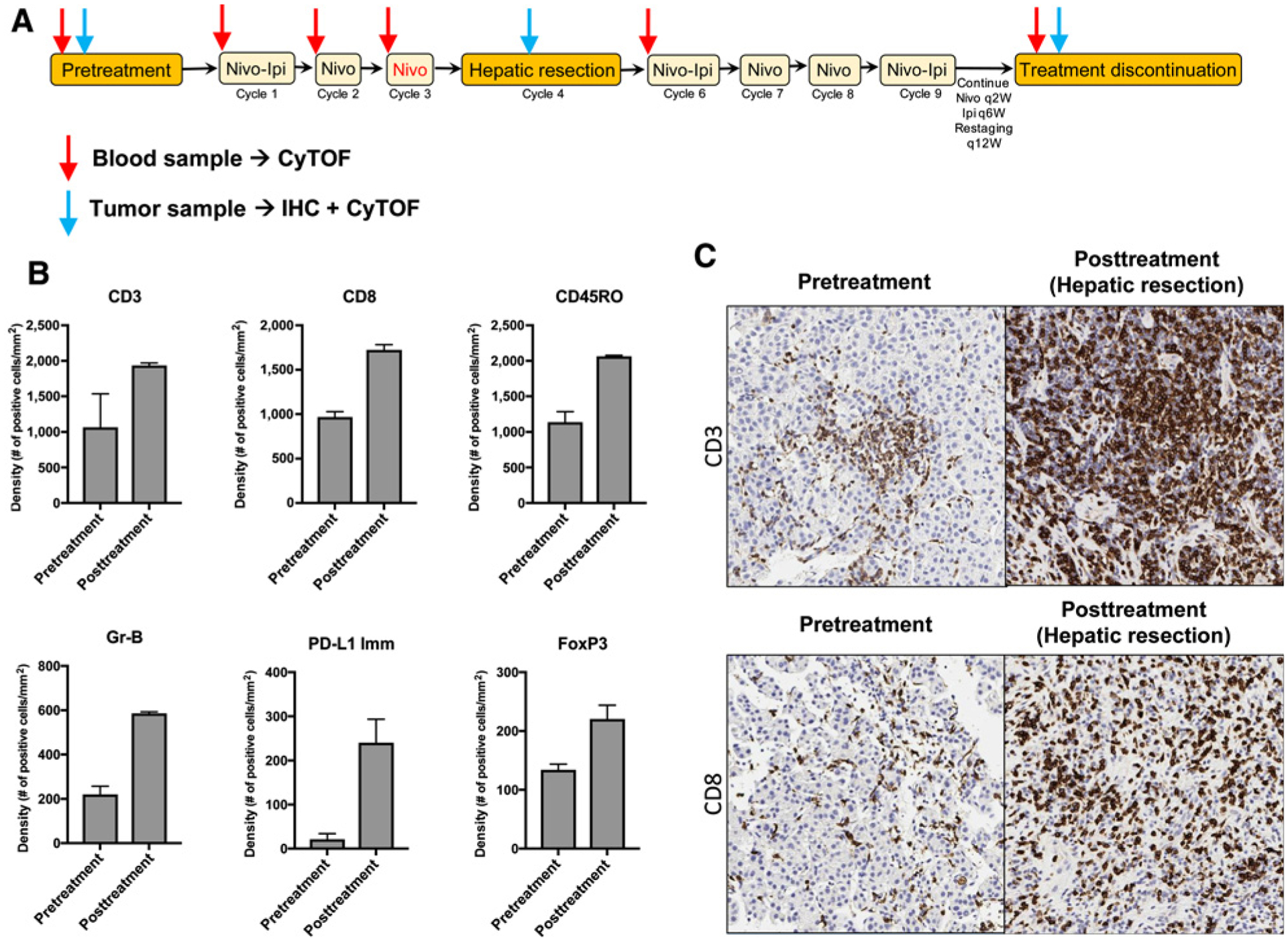
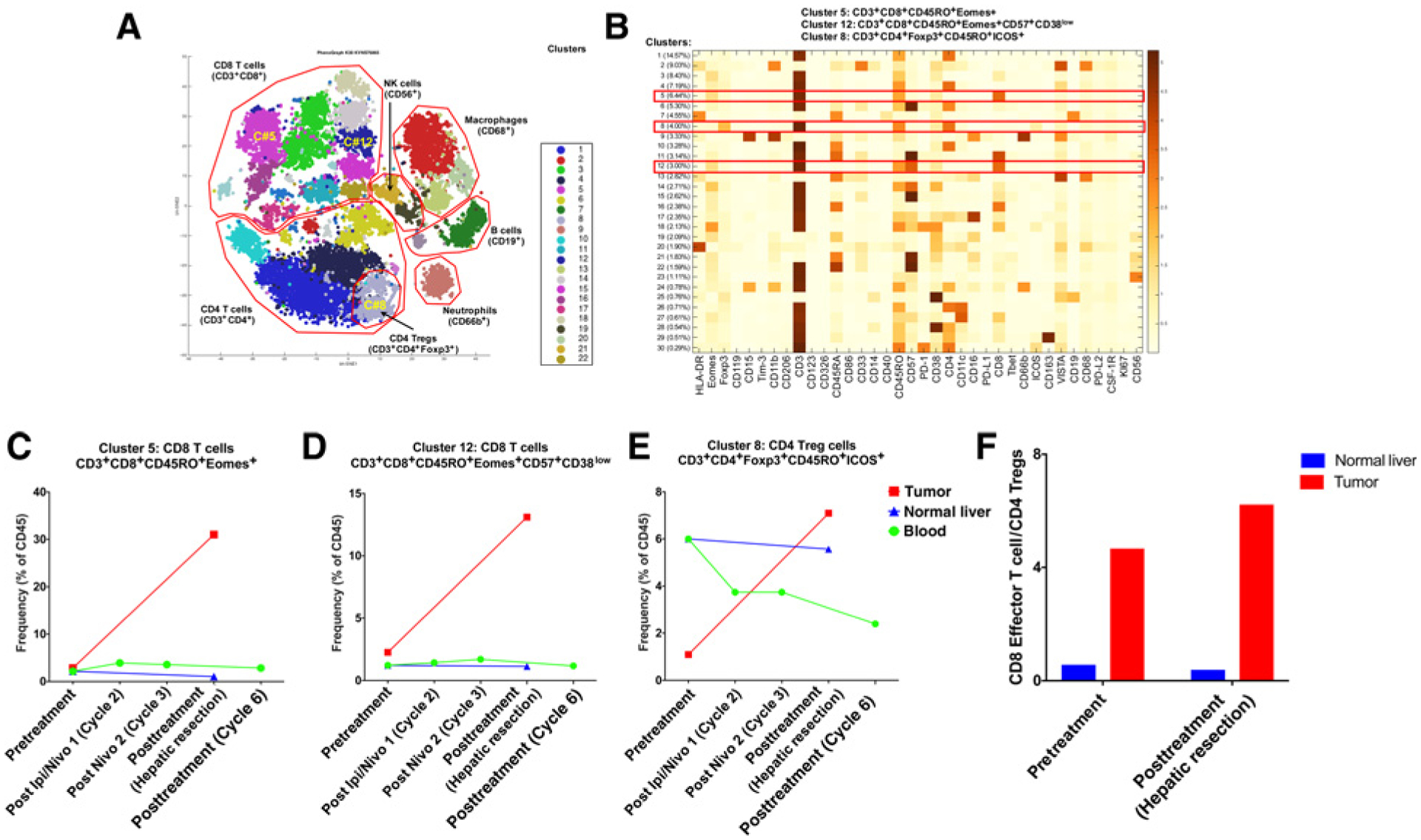
In hepatocellular carcinoma (HCC), surgical resection is associated with high recurrence rate, and no effective adjuvant therapy currently exists. We initiated a pilot randomized trial of perioperative immunotherapy with nivolumab and ipilimumab for resectable HCC. Here, we provide an illustrative report of a case that achieved a complete response and report immunologic correlates of this complete pathologic response to perioperative immunotherapy. Clinical response was correlated with an increase in CD8+ T-cell infiltration, with an increase in two effector T-cell clusters. This study is ongoing, and the final results may contribute to a paradigm shift in the perioperative treatment of HCC, leading to the incorporation of immunotherapy in the curative setting.
©2019 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest
P. Sharma has ownership interest (including stock, patents, etc.) in Jounce, Neon, Constellation, Forty Seven, and is a consultant/advisory board member for Jounce, Neon, Marker, Pieris, Imaginab, Constellation, Forty Seven, Optera, Hummingbird, BioAtla, Codiak, Polaris, and Oncolytics. No potential conflicts of interest were disclosed by the other authors.
Figures

References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin 2015;65:87–108. - PubMed
-
- Bruix J, Takayama T, Mazzaferro V, Chau G-Y, Yang J, Kudo M, et al. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): a phase 3, randomised, double-blind, placebo-controlled trial. Lancet Oncol 2015;16:1344–54. - PubMed
-
- Zhu AX, Finn RS, Edeline J, Cattan S, Ogasawara S, Palmer D, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol 2018;19:940–52. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
