

How thoracic surgeon manage tracheal tumors in African country? (Case series)
- PMID: 31289669
- PMCID: PMC6593208
- DOI: 10.1016/j.amsu.2019.06.007
How thoracic surgeon manage tracheal tumors in African country? (Case series)
Abstract
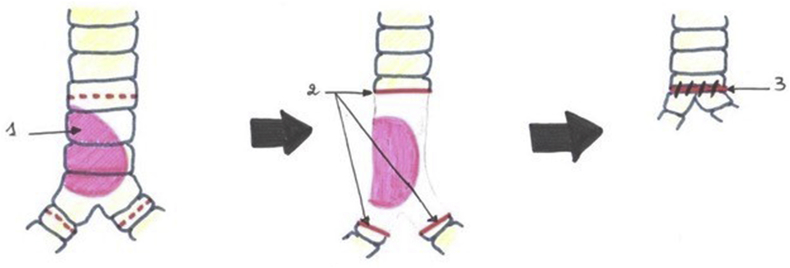
Introduction: Tracheal tumors are a rare pathological entity whose diagnosis is usually delayed by clinical latency. Surgery, which consists of a tracheal resection-anastomosis with or without reconstructive reconstruction, remains the treatment that ensures the best long-term survival.
Methods: This is a retrospective study about 8 patients admitted in the department of thoracic surgery of Hassan II's university hospital of Fes for tracheal tumors management during 7 years time (December 2010 to December 2017).
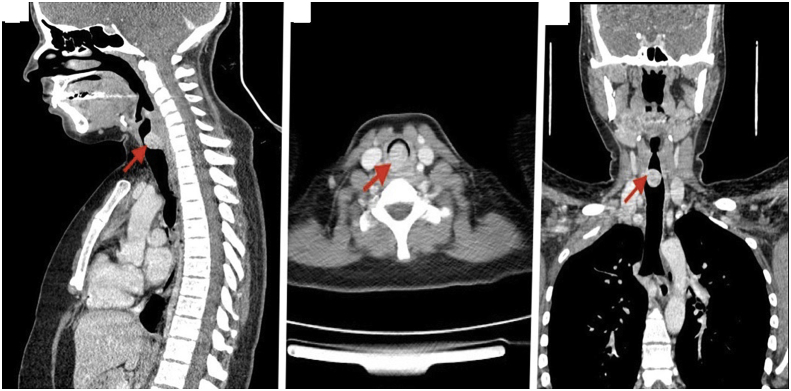
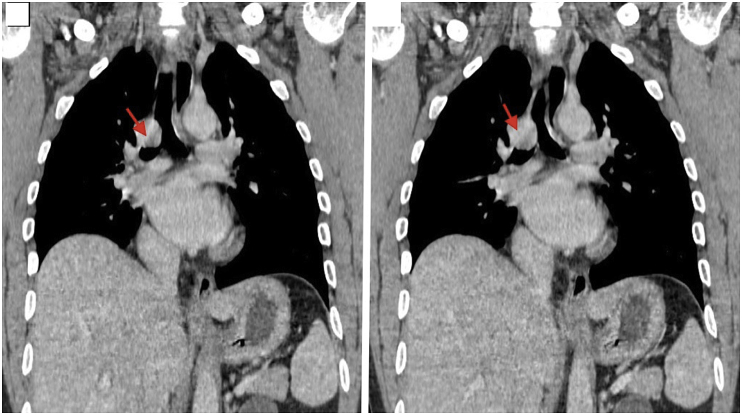
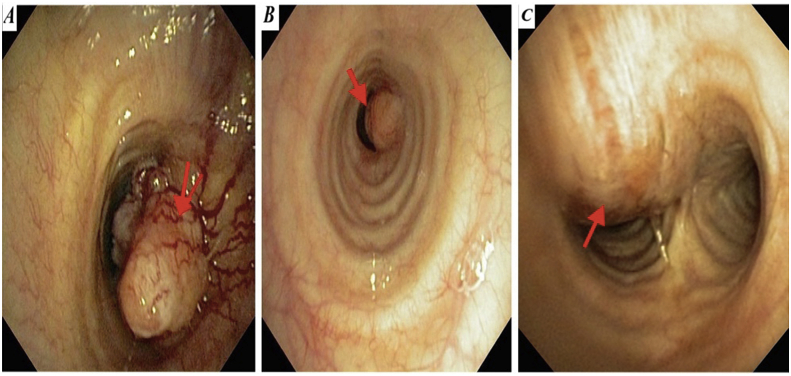
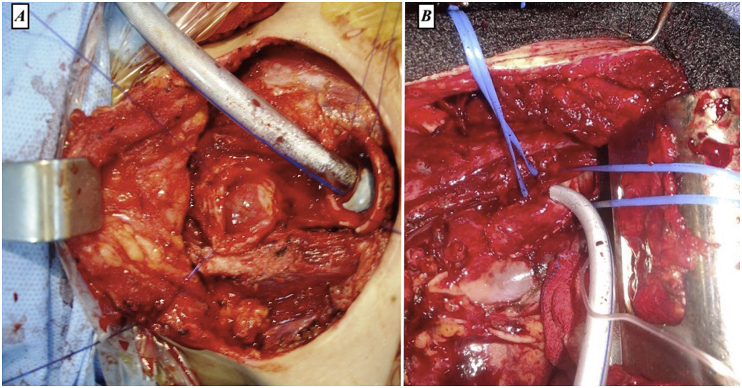
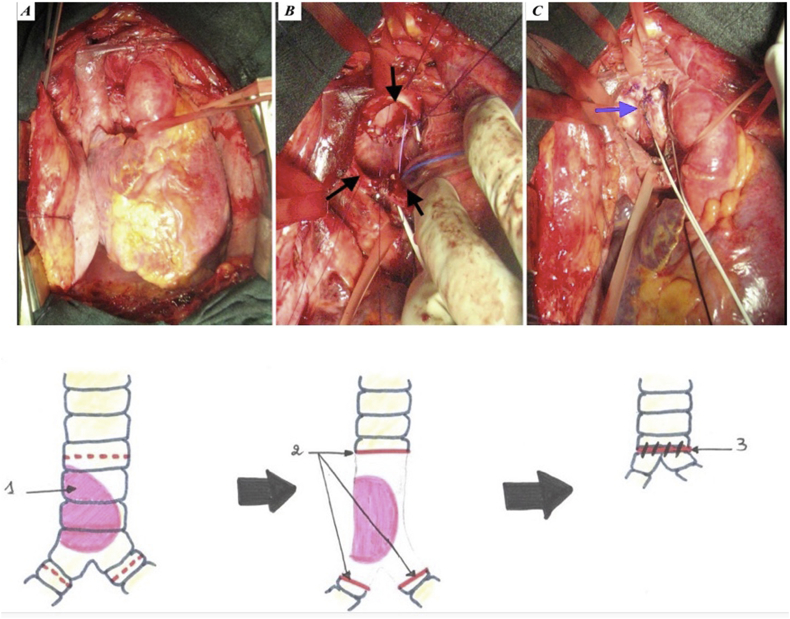
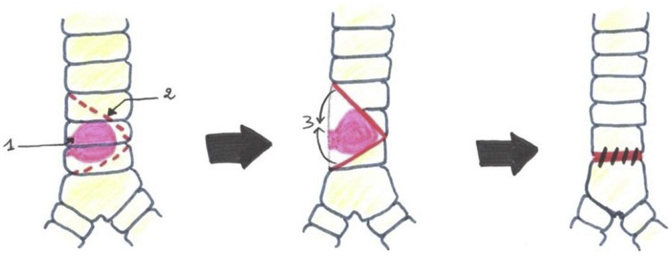
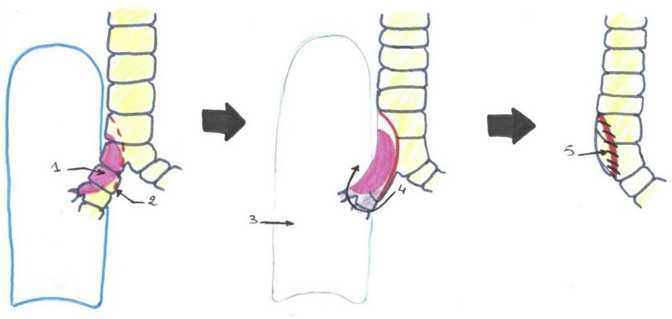
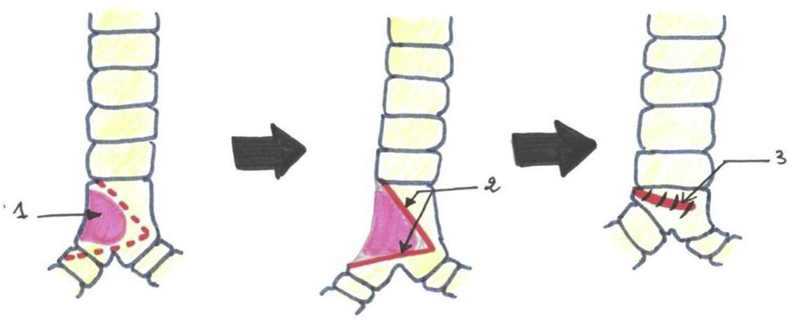
Results: There were 6 men and 2 women with an average age of 44.4 years ranged from 17 to 65 years, 4 were smokers. Dyspnea was the main trigger sign. Seven (7) have undergone bronchial fibroscopy diagnostic with a finding of budding process in 5 patients, the middle of the trachea is often concerned in 3 patients, obstructing the lumen of the trachea in almost all patients. The treatment in all patients was surgical with an intubation via the operative field, 4 trachea resection-anastomosis, 4 plasty (Lateral resection with V plasty, Kergin's plasty, Mattey's tracheobronchial anastomosis and widened V-resection to the carina). The most common histological type in our series was Adenoid Cystic Carcinoma in 2 of our patients. For the other patients we have found squamous cell carcinoma (1 case), adenocarcinoma (1 case), atypical carcinoid tumor (1 case), low grade mucoepidermoid carcinoma (1 case), an adenoma pleomorph (1 case) and endotracheal goiter (1 case). The operative follow-up was simple in 7 of our patients, all of whom underwent post-operative fibroscopy within an average of 9 days. Two cases of post-operative recurrent palsy had been observed, all of which had progressed well under treatment. We have noted 2 deaths, including one at day 4 post-operative, and the other died from complications of post-radiation tracheal stenosis. Back to 32 months' average follow-up, we have enregistered a case of a distant relapse by cervical lymph node metastasis in one patient, 5 years after surgery.
Conclusion: Primary tumors of the trachea remain of reserved prognosis with 5-year survival of 57% of all histological types combined. Computed tomodensitometry and tracheobronchial fibroscopy remain the means of reference exploration in the diagnosis and assessment of surgical resectability.
Keywords: Adenoid cystic carcinoma; Rigid bronchoscopy; Surgery; Tracheal endoprosthesis; Tracheal stenosis; Tracheal tumors.
Figures


Similar articles
-
[Malignant tracheal tumors--surgical experiences in 6 patients with primary malignancies of the trachea. Current diagnosis and therapy].Langenbecks Arch Chir. 1996;381(1):23-33. doi: 10.1007/BF00184251. Langenbecks Arch Chir. 1996. PMID: 8717171 German.
-
[Surgery for primary adenoid cystic carcinoma of cervical trachea].Ai Zheng. 2004 May;23(5):581-3. Ai Zheng. 2004. PMID: 15142459 Chinese.
-
Resection of the Tracheobronchial Bifurcation With Complete Preservation of Lung Parenchyma.Ann Thorac Surg. 2017 Nov;104(5):1741-1747. doi: 10.1016/j.athoracsur.2017.05.053. Epub 2017 Sep 19. Ann Thorac Surg. 2017. PMID: 28935346
-
[Primary tracheal tumors of the neck and mediastinum : resection and reconstruction procedures].Chirurg. 2011 Feb;82(2):125-33. doi: 10.1007/s00104-010-1974-7. Chirurg. 2011. PMID: 21253678 Review. German.
-
Adenoid cystic carcinoma of the trachea: a clinico-pathological analysis.Pan Afr Med J. 2015 Mar 13;20:240. doi: 10.11604/pamj.2015.20.240.3953. eCollection 2015. Pan Afr Med J. 2015. PMID: 27386036 Free PMC article. Review.
References
-
- Heffner D.K. Diseases of the trachea. In: Barnes L., editor. Surgical Pathology of the Head and Neck. 2ndedition. Marcel Dekker; New York: 2001. pp. 602–631.
-
- Webb B.D., Walsh G.L., Roberts D.B., Sturgis E.M. Primary tracheal malignant neoplasms: the university of Texas MD Anderson cancer center experience. J. Am. Coll. Surg. 2006;202:237—46. - PubMed
-
- Soualhi M., El Ouazani H., Benamor J., Chaibainou A., FassyFihri M.T., Benosman A. Carcinome adénoïde kystique trachéal A propos de trois cas. Rev. Pneumol. Clin. 2003;59(4):197–200. - PubMed
-
- Gaissert H.A., Honings J., Gokhale M. Treatment of tracheal tumors. Semin. Thorac. Cardiovasc. Surg. 2009;21(3):290–295. - PubMed
-
- Agha R.A., Borrelli M.R., Farwana R., Koshy K., Fowler A., Orgill D.P., For the PROCESS Group The PROCESS 2018 statement: updating consensus preferred reporting of case series in surgery (PROCESS) guidelines. Int. J. Surg. 2018;60:279–282. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
