

Single systemic transfer of a human gene associated with exceptional longevity halts the progression of atherosclerosis and inflammation in ApoE knockout mice through a CXCR4-mediated mechanism
- PMID: 31289820
- PMCID: PMC7340354
- DOI: 10.1093/eurheartj/ehz459
Single systemic transfer of a human gene associated with exceptional longevity halts the progression of atherosclerosis and inflammation in ApoE knockout mice through a CXCR4-mediated mechanism
Abstract
Aims: Here, we aimed to determine the therapeutic effect of longevity-associated variant (LAV)-BPIFB4 gene therapy on atherosclerosis.
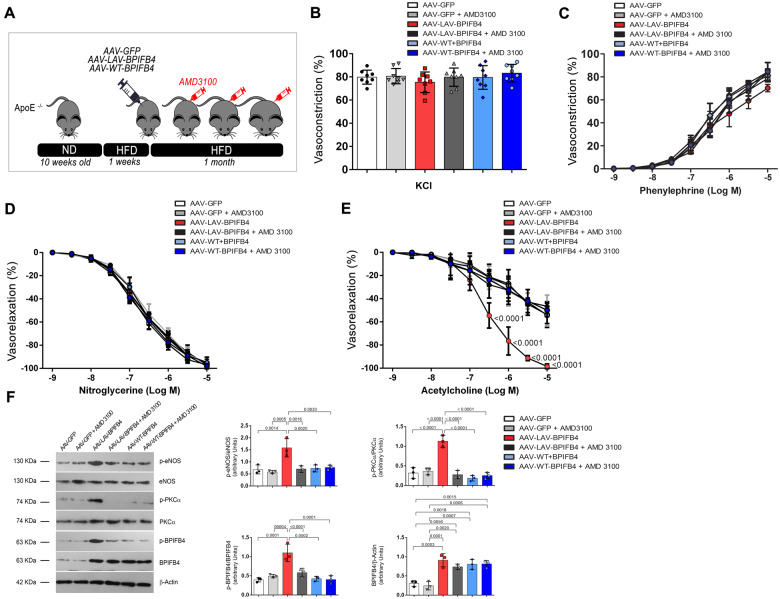
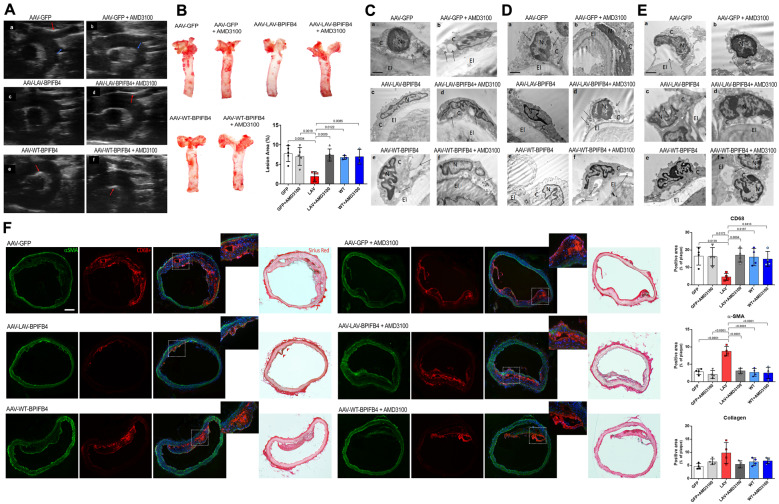
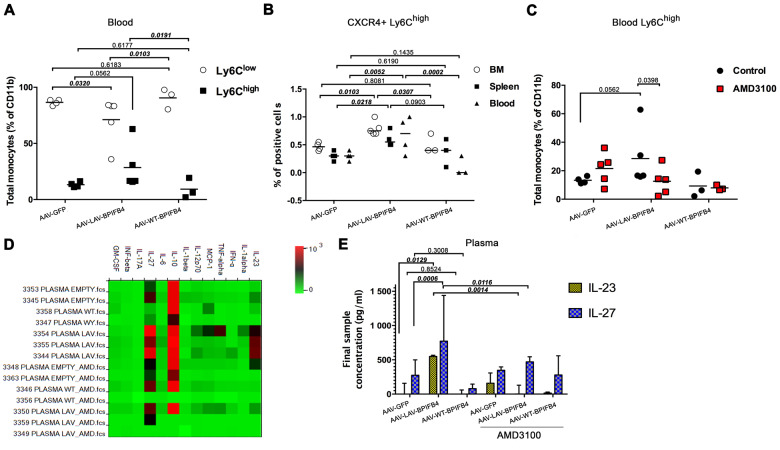
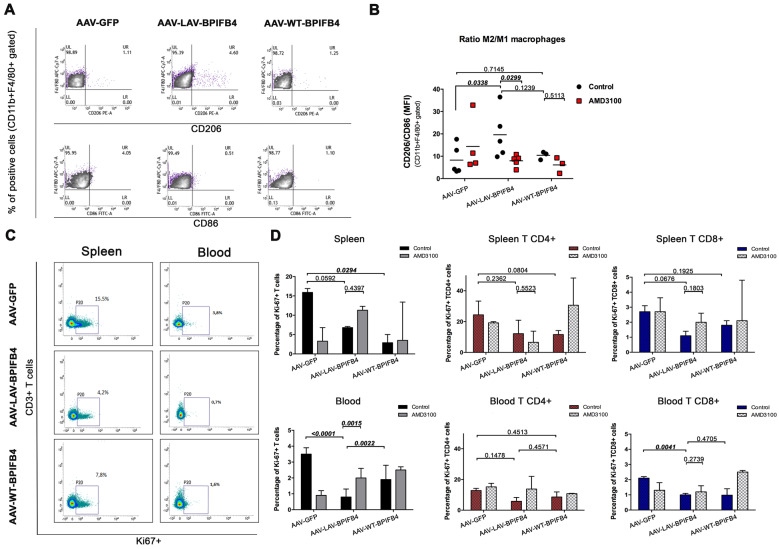
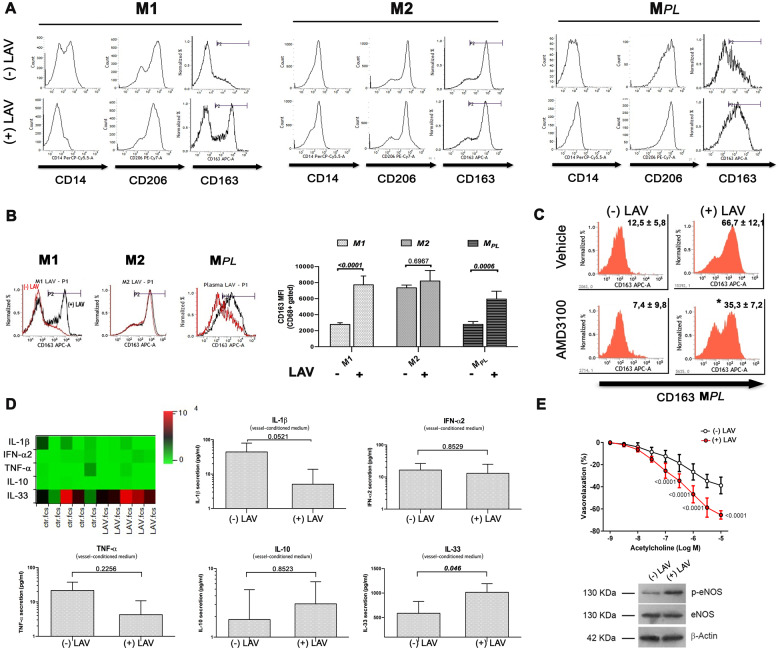
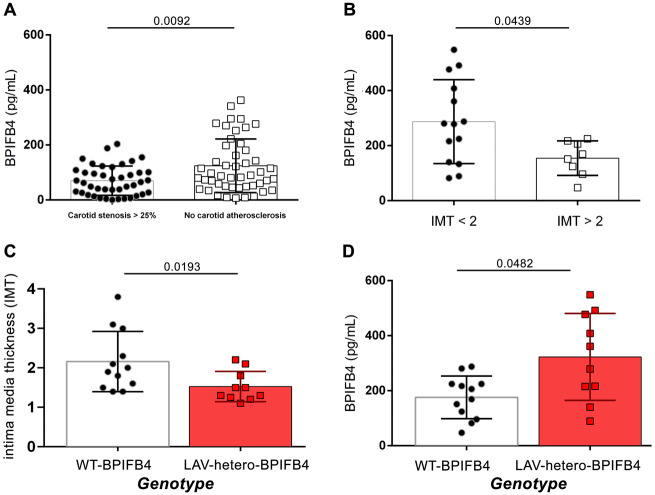
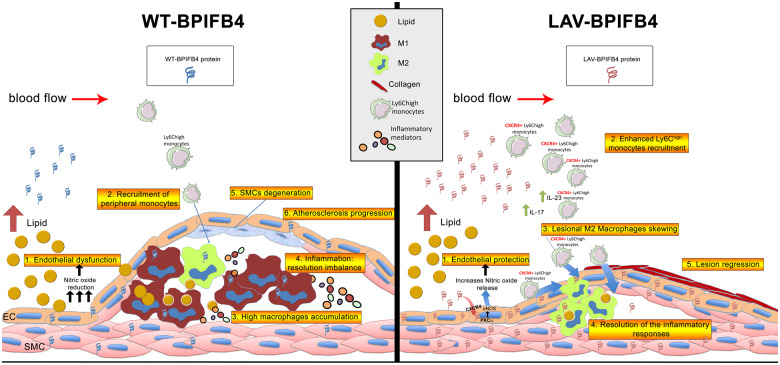
Methods and results: ApoE knockout mice (ApoE-/-) fed a high-fat diet were randomly allocated to receive LAV-BPIFB4, wild-type (WT)-BPIFB4, or empty vector via adeno-associated viral vector injection. The primary endpoints of the study were to assess (i) vascular reactivity and (ii) atherosclerotic disease severity, by Echo-Doppler imaging, histology and ultrastructural analysis. Moreover, we assessed the capacity of the LAV-BPIFB4 protein to shift monocyte-derived macrophages of atherosclerotic mice and patients towards an anti-inflammatory phenotype. LAV-BPIFB4 gene therapy rescued endothelial function of mesenteric and femoral arteries from ApoE-/- mice; this effect was blunted by AMD3100, a CXC chemokine receptor type 4 (CXCR4) inhibitor. LAV-BPIFB4-treated mice showed a CXCR4-mediated shift in the balance between Ly6Chigh/Ly6Clow monocytes and M2/M1 macrophages, along with decreased T cell proliferation and elevated circulating levels of interleukins IL-23 and IL-27. In vitro conditioning with LAV-BPIFB4 protein of macrophages from atherosclerotic patients resulted in a CXCR4-dependent M2 polarization phenotype. Furthermore, LAV-BPIFB4 treatment of arteries explanted from atherosclerotic patients increased the release of atheroprotective IL-33, while inhibiting the release of pro-inflammatory IL-1β, inducing endothelial nitric oxide synthase phosphorylation and restoring endothelial function. Finally, significantly lower plasma BPIFB4 was detected in patients with pathological carotid stenosis (>25%) and intima media thickness >2 mm.
Conclusion: Transfer of the LAV of BPIFB4 reduces the atherogenic process and skews macrophages towards an M2-resolving phenotype through modulation of CXCR4, thus opening up novel therapeutic possibilities in cardiovascular disease.
Keywords: Atherosclerosis; Immune system; Low-density lipoprotein; Vascular function.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Longevity-associated gene variant halts progression of atherosclerosis.Nat Rev Cardiol. 2019 Sep;16(9):516. doi: 10.1038/s41569-019-0243-9. Nat Rev Cardiol. 2019. PMID: 31332350 No abstract available.
-
Longevity-associated variant BPIFB4 gene transfer to recapitulate healthy ageing in patients at risk: is the future around the corner?Eur Heart J. 2020 Jul 7;41(26):2498-2500. doi: 10.1093/eurheartj/ehz522. Eur Heart J. 2020. PMID: 31332429 No abstract available.
References
-
- Ridker PM, Everett BM, Thuren T, MacFadyen JG, Chang WH, Ballantyne C, Fonseca F, Nicolau J, Koenig W, Anker SD, Kastelein JJP, Cornel JH, Pais P, Pella D, Genest J, Cifkova R, Lorenzatti A, Forster T, Kobalava Z, Vida-Simiti L, Flather M, Shimokawa H, Ogawa H, Dellborg M, Rossi PRF, Troquay RPT, Libby P, Glynn RJ, Group CT.. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med 2017;377:1119–1131. - PubMed
-
- Jin DK, Shido K, Kopp HG, Petit I, Shmelkov SV, Young LM, Hooper AT, Amano H, Avecilla ST, Heissig B, Hattori K, Zhang F, Hicklin DJ, Wu Y, Zhu Z, Dunn A, Salari H, Werb Z, Hackett NR, Crystal RG, Lyden D, Rafii S.. Cytokine-mediated deployment of SDF-1 induces revascularization through recruitment of CXCR4+ hemangiocytes. Nat Med 2006;12:557–567. - PMC - PubMed
-
- Shantsila E, Tapp LD, Wrigley BJ, Montoro-García S, Lip GYH.. CXCR4 positive and angiogenic monocytes in myocardial infarction. Thromb Haemost 2013;109:255–262. - PubMed
-
- Chong SZ, Evrard M, Devi S, Chen J, Lim JY, See P, Zhang Y, Adrover JM, Lee B, Tan L, Li JL, Liong KH, Phua C, Balachander A, Boey A, Liebl D, Tan SM, Chan JK, Balabanian K, Harris JE, Bianchini M, Weber C, Duchene J, Lum J, Poidinger M, Chen Q, Renia L, Wang CI, Larbi A, Randolph GJ, Weninger W, Looney MR, Krummel MF, Biswas SK, Ginhoux F, Hidalgo A, Bachelerie F, Ng LG.. CXCR4 identifies transitional bone marrow premonocytes that replenish the mature monocyte pool for peripheral responses. J Exp Med 2016;213:2293–2314. - PMC - PubMed
