

Long-term Reintervention After Endovascular Abdominal Aortic Aneurysm Repair
- PMID: 31290764
- PMCID: PMC10683776
- DOI: 10.1097/SLA.0000000000003446
Long-term Reintervention After Endovascular Abdominal Aortic Aneurysm Repair
Abstract
Objective: To describe the long-term reintervention rate after endovascular abdominal aortic aneurysm repair (EVR), and identify factors predicting reintervention.
Summary of background data: EVR is the most common method of aneurysm repair in America, and reintervention after EVR is common. Clinical factors predicting reintervention have not been described in large datasets with long-term follow-up.
Methods: We studied patients who underwent EVR using the Vascular Quality Initiative registry linked to Medicare claims. Our primary outcome was reintervention, defined as any procedure related to the EVR after discharge from the index hospitalization. We used classification and regression tree modeling to inform a multivariable Cox-regression model predicting reintervention after EVR.
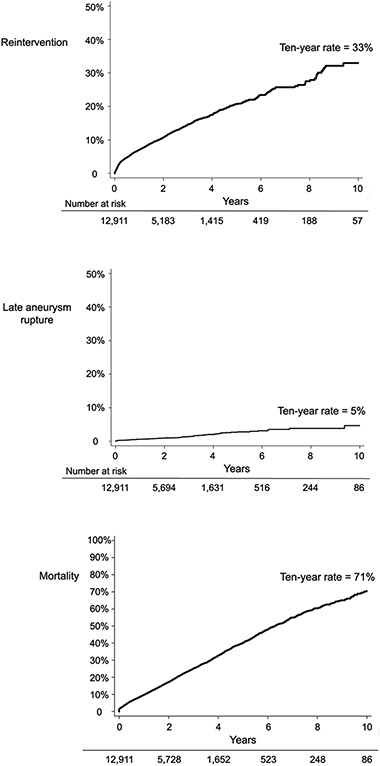
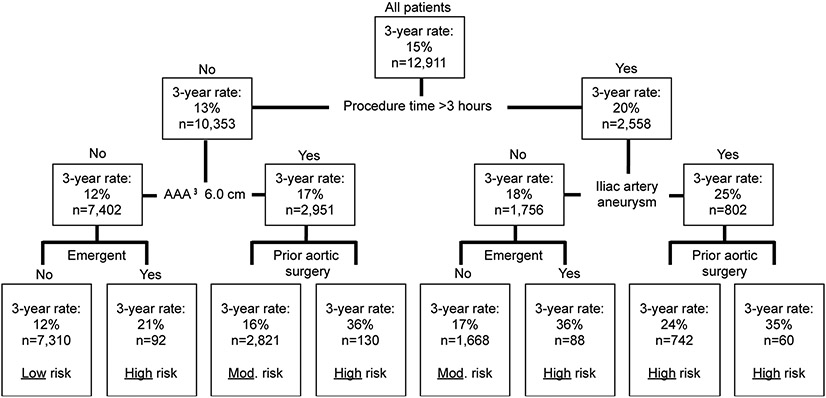
Results: We studied 12,911 patients treated from 2003 to 2015. Mean age was 75.5 ± 7.3 years, 79.9% were male, and 89.1% of operations were elective. The 3-year reintervention rate was 15%, and the 10-year rate was 33%. Five factors predicted reintervention: operative time ≥3.0 hours, aneurysm diameter ≥6.0 cm, an iliac artery aneurysm ≥2.0 cm, emergency surgery, and a history of prior aortic surgery. Patients with no risk factors had a 3-year reintervention rate of 12%, and 10-year rate of 26% (n = 7310). Patients with multiple risk factors, such as prior aortic surgery and emergent surgery, had a 3-year reintervention rate 72%, (n = 32). Modifiable factors including EVR graft manufacturer or supra-renal fixation were not associated with reintervention (P = 0.76 and 0.79 respectively).
Conclusions: All patients retain a high likelihood of reintervention after EVR, but clinical factors at the time of repair can predict those at highest risk.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
Figures
References
-
- Patel R, Sweeting MJ, Powell JT, et al. Endovascular versus open repair of abdominal aortic aneurysm in 15-years' follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): a randomised controlled trial. The Lancet 2016; 388(10058):2366–2374. - PubMed
-
- Qadura M, Pervaiz F, Harlock JA, et al. Mortality and reintervention following elective abdominal aortic aneurysm repair. J Vasc Surg 2013; 57(6):1676–83, 1683 e1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
