

Development and Validation of a Bedside Risk Assessment for Sustained Prescription Opioid Use After Surgery
- PMID: 31290987
- PMCID: PMC6624809
- DOI: 10.1001/jamanetworkopen.2019.6673
Development and Validation of a Bedside Risk Assessment for Sustained Prescription Opioid Use After Surgery
Abstract
Importance: The increased use of prescription opioid medications has contributed to an epidemic of sustained opioid use, misuse, and addiction. Adults of working age are thought to be at greatest risk for prescription opioid dependence.
Objective: To develop a risk score (the Stopping Opioids After Surgery score) for sustained prescription opioid use after surgery in a working-age population using readily available clinical information.
Design, setting, and participants: In this case-control study, claims from TRICARE (the insurance program of the US Department of Defense) for working-age adult (age 18-64 years) patients undergoing 1 of 10 common surgical procedures from October 1, 2005, to September 30, 2014, were queried. A logistic regression model was used to identify variables associated with sustained prescription opioid use. The point estimate for each variable in the risk score was determined by its β coefficient in the model. The risk score for each patient represented the summed point totals, ranging from 0 to 100, with a lower score indicating lower risk of sustained prescription opioid use. Data were analyzed from September 25, 2018, to February 5, 2019.
Exposures: Exposures were age; race; sex; marital status; socioeconomic status; discharge disposition; procedure intensity; length of stay; intensive care unit admission; comorbid diabetes, liver disease, renal disease, malignancy, depression, or anxiety; and prior opioid use status.
Main outcomes and measures: The primary outcome was sustained prescription opioid use, defined as uninterrupted use for 6 months following surgery. A risk score for each patient was calculated and then used as a predictor of sustained opioid use after surgical intervention. The area under the curve and the Brier score were used to determine the accuracy of the scoring system and the Hosmer-Lemeshow goodness-of-fit test was used to evaluate model calibration.
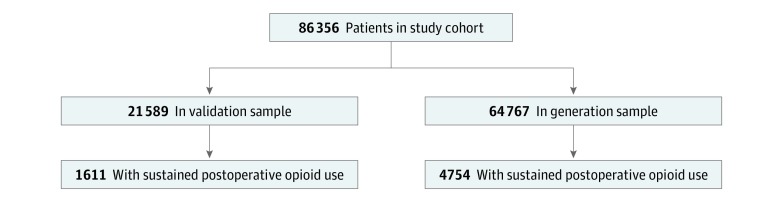
Results: Of 86 356 patients in the analysis (48 827 [56.5%] male; mean [SD] age, 46.5 [14.5] years), 6365 (7.4%) met criteria for sustained prescription opioid use. The sample used for model generation consisted of 64 767 patients, while the validation sample had 21 589 patients. Prior opioid exposure was the factor most strongly associated with sustained opioid use (odds ratio, 13.00; 95% CI, 11.87-14.23). The group with the lowest scores (<31) had a mean (SD) 4.1% (2.5%) risk of sustained opioid use; those with intermediate scores (31-50) had a mean (SD) risk of 14.9% (6.3%); and those with the highest scores (>50) had a mean (SD) risk of 35.8% (3.6%).
Conclusions and relevance: This study developed an intuitive and accessible opioid risk assessment applicable to the care of working-age patients following surgery. This tool is scalable to clinical practice and can potentially be incorporated into electronic medical record platforms to enable automated calculation and clinical alerts that are generated in real time.
Conflict of interest statement
Figures
Comment in
-
Three Critical Questions That Should Be Asked Before Using Prediction Models for Clinical Decision Support.JAMA Netw Open. 2019 Jul 3;2(7):e196661. doi: 10.1001/jamanetworkopen.2019.6661. JAMA Netw Open. 2019. PMID: 31290984 No abstract available.
References
-
- Paulozzi LJ, Mack KA, Hockenberry JM; Division of Unintentional Injury Prevention, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention . Vital signs: variation among States in prescribing of opioid pain relievers and benzodiazepines—United States, 2012. MMWR Morb Mortal Wkly Rep. 2014;63(26):563-568. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
