

Management and referral for high-risk conditions and complications during the antenatal period: knowledge, practice and attitude survey of providers in rural public healthcare in two states of India
- PMID: 31291968
- PMCID: PMC6617826
- DOI: 10.1186/s12978-019-0765-y
Management and referral for high-risk conditions and complications during the antenatal period: knowledge, practice and attitude survey of providers in rural public healthcare in two states of India
Abstract
Background: Appropriate antenatal care improves pregnancy outcomes. Routine antenatal care is provided at primary care facilities in rural India and women at-risk of poor outcomes are referred to advanced centres in cities. The primary care facilities include Sub-health centres, Primary health centres, and Community health centres, in ascending order of level of obstetric care provided. The latter two should provide basic and comprehensive obstetric care, respectively, but they provide only partial services. In such scenario, the management and referrals during pregnancy are less understood. This study assessed rural providers' perspectives on management and referrals of antenatal women with high obstetric risk, or with complications.
Methods: We surveyed 147 health care providers in primary level public health care from poor and better performing districts from two states. We assessed their knowledge, attitudes and practices regarding obstetric care, referral decisions and pre-referral treatments provided for commonly occurring obstetric high-risk conditions and complications.
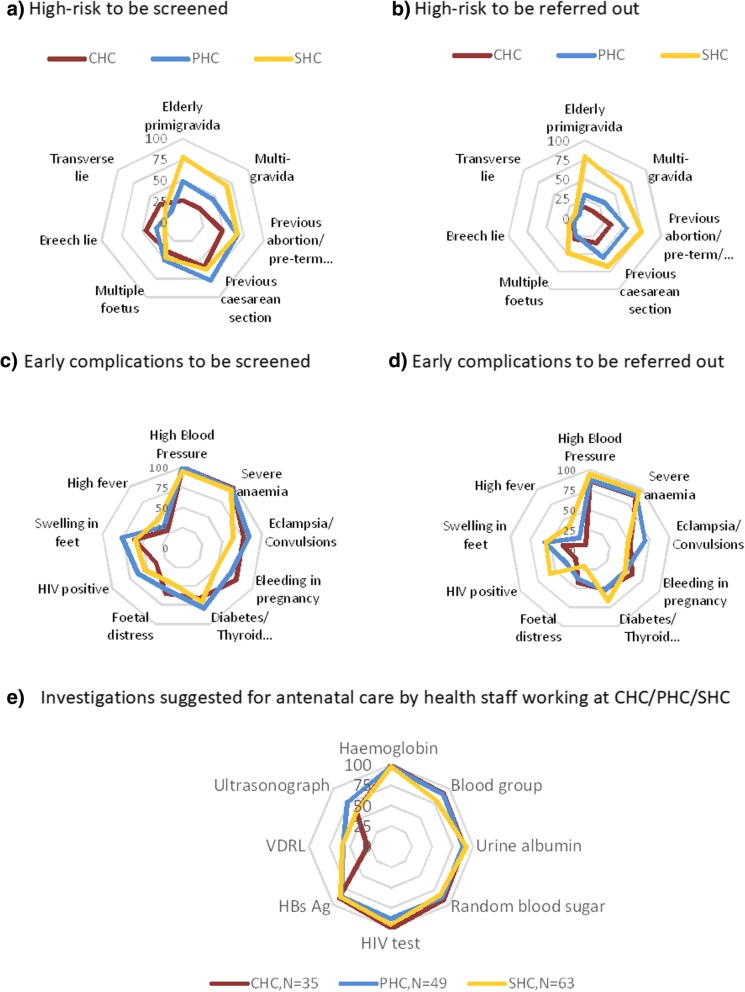
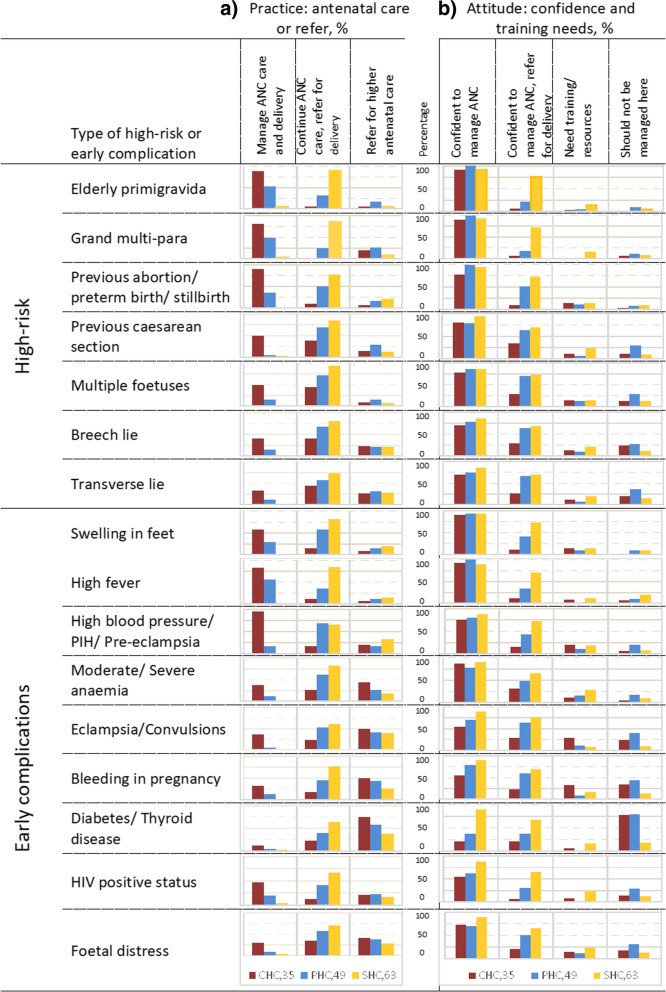
Results: Staff had sub-optimal knowledge of, and practices for, screening common high-risk conditions and assessing complications in pregnancy. Only 31% (47/147) mentioned screening for at least 10 of the 16 common high-risk conditions and early complications of pregnancy. Only 35% (17/49) of the staff at Primary health centres, and 51% (18/35) at Community health centres, mentioned that they managed these conditions and, the remaining staff referred most of such cases early in pregnancy. The staff mentioned inability to manage childbirth of women with high-risk conditions and complications. Thus in absence of efficient referral systems and communication, it was better for these women to receive antenatal care at the advanced centres (often far) where they should deliver. There were large gaps in knowledge of emergency treatment for obstetric complications in pregnancy and pre-referral first-aid. Staff generally were low on confidence and did not have adequate resources. Nurses had limited roles in decision making. Staff desired skill building, mentoring, moral support, and motivation from senior officers.
Conclusion: The Indian health system should improve the provision of obstetric care by standardising services at each level of health care and increasing the focus on emergency treatment for complications, appropriate decision-making for referral, and improving referral communication and staff support.
Keywords: Maternity services; Obstetric; Obstetric complication; Obstetric high-risk; Pregnancy; Pregnant women; Quality.
Conflict of interest statement
The authors declared that they have no competing interests.
Figures

References
-
- WHO . Maternal mortality: key facts [internet] 2018.
-
- WHO. Trends in maternal mortality: 1990 to 2015: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations population division. Geneva; 2015.
-
- Registrar General of India. Special bulletin on maternal mortality in India 2014–16: sample registration system: New Delhi; 2018.
-
- Department of Economic and Social Affairs. Sustainable Development Goal 3. United Nations. 2018.
-
- UNICEF, DIFID. Maternal and perinatal death enquiry and response: New Delhi; 2008.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
