

Network meta-analysis comparing neoadjuvant chemoradiation, neoadjuvant chemotherapy and upfront surgery in patients with resectable, borderline resectable, and locally advanced pancreatic ductal adenocarcinoma
- PMID: 31291998
- PMCID: PMC6617703
- DOI: 10.1186/s13014-019-1330-0
Network meta-analysis comparing neoadjuvant chemoradiation, neoadjuvant chemotherapy and upfront surgery in patients with resectable, borderline resectable, and locally advanced pancreatic ductal adenocarcinoma
Abstract
Purpose: Neoadjuvant chemoradiation or chemotherapy has improved the treatment efficacy of patients with resectable, borderline resectable, and locally advanced pancreatic ductal adenocarcinoma (PDAC). Due to the optimal regimen remains inconclusive, we aimed to compare these treatments in terms of margin negative (R0) resection rate and overall survival (OS) with Bayesian analysis.
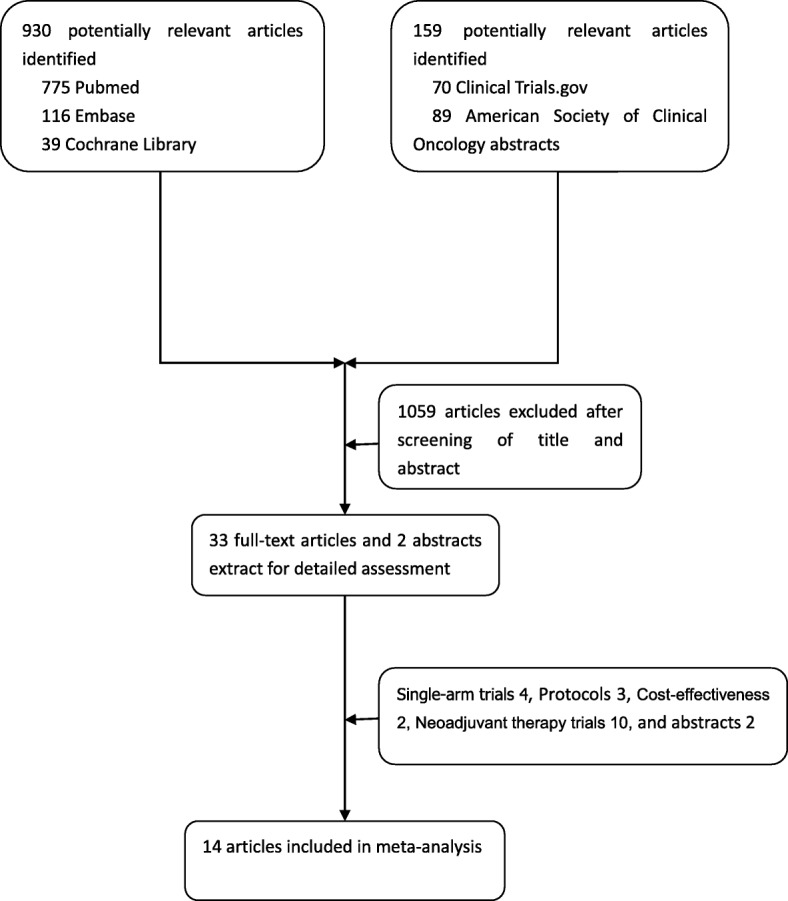
Patients and methods: We reviewed literature titles and abstracts comparing three treatment strategies (neoadjuvant chemoradiation, neoadjuvant chemotherapy, and upfront surgery) in PubMed, Embase, Cochrane Library, the American Society of Clinical Oncology and ClinicalTrials.gov database from 2009 to 2018 to estimate relative odds ratios (ORs) for margin negative (R0) resection rate and hazard ratios (HRs) for overall survival (OS) in all include trials.
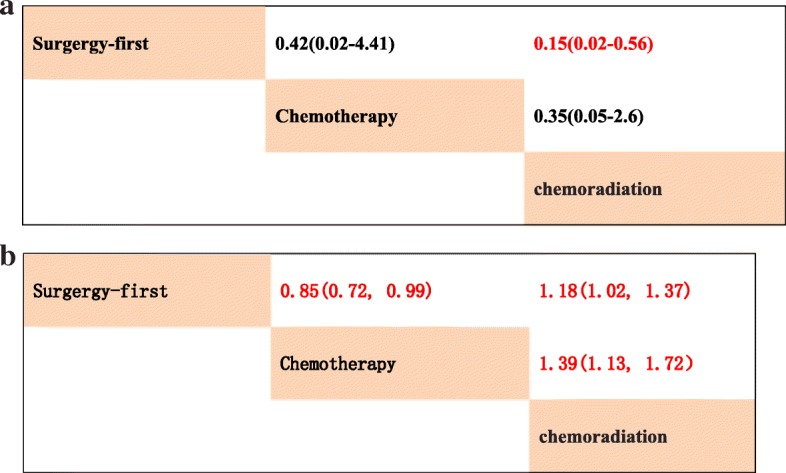
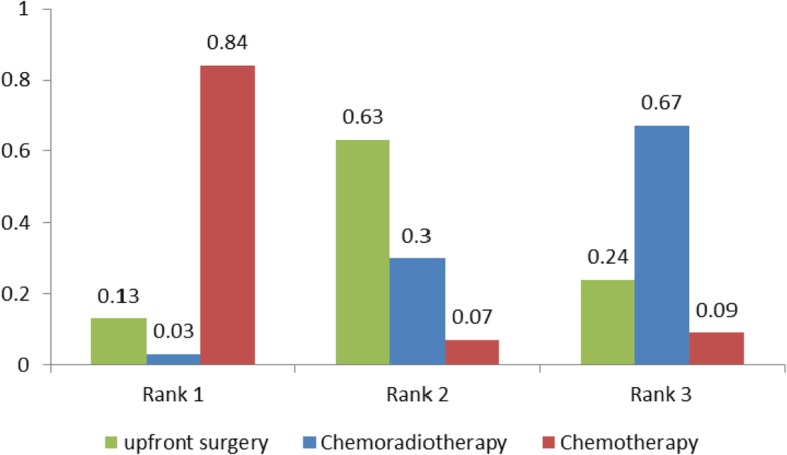
Results: A total of 14 literatures with 1056 patients were enrolled in this Bayesian analysis. In the pairwise meta-analysis from limited head-to-head studies, compared with neoadjuvant chemotherapy, neoadjuvant chemoradiation showed superior OS significantly (HR 0.8, 95% CI 0.60-0.99, p < 0.001) and there was no significant difference in R0 resection rate (OR 1.02, 95%CI 0.45-2.33, I2 = 34.6%). However, in the network meta-analysis from all enrolled clinical trials, neoadjuvant chemoradiation showed significantly higher R0 resection rate over upfront surgery (HR 0.15, 95% CrI 0.02-0.56), whereas neoadjuvant chemotherapy did not provide better efficacy in R0 resection over upfront surgery (HR 0.42, 95% CrI 0.02-4.41). For R0 resection rate, neoadjuvant chemoradiation has the highest probability of ranking one compared with neoadjuvant chemotherapy or upfront surgery (79% vs 21% vs 0%). For OS, neoadjuvant chemotherapy has the highest probability of ranking one compared with neoadjuvant chemoradiation or upfront surgery (98% vs 0% vs 2%). Neoadjuvant chemotherapy was associated with higher rates of postoperative complications (rank worst: 84%), followed by neoadjuvant chemoradiotherapy (13%) and upfront surgery (3%).
Conclusions: Different neoadjuvant treatment was selected based on various purposes, whether increasing R0 resection rate or not. Future clinical trials comparing neoadjuvant chemoradiation with neoadjuvant chemotherapy are warranted to confirm our results.
Keywords: Bayesian analysis; Neoadjuvant therapy; Network meta-analysis; Pancreatic ductal adenocarcinoma.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67(1):7–30. - PubMed
-
- Malvezzi M, Carioli G, Bertuccio P, Boffetta P, et al. European cancer mortality predictions for the year 2017, with focus on lung cancer. Ann Oncol. 2017;28(5):1117–1123. - PubMed
-
- Abrams RA, Lowy AM, O'Reilly EM, Wolff RA, et al. Combined modality treatment of resectable and borderline resectable pancreas cancer: expert consensus statement. Ann Surg Oncol. 2009;16(7):1751–1756. - PubMed
-
- Callery MP, Chang KJ, Fishman EK, Talamonti MS, et al. Pretreatment assessment of resectable and borderline resectable pancreatic cancer: expert consensus statement. Ann Surg Oncol. 2009;16(7):1727–1733. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
