

GFR Slope as a Surrogate End Point for Kidney Disease Progression in Clinical Trials: A Meta-Analysis of Treatment Effects of Randomized Controlled Trials
- PMID: 31292197
- PMCID: PMC6727261
- DOI: 10.1681/ASN.2019010007
GFR Slope as a Surrogate End Point for Kidney Disease Progression in Clinical Trials: A Meta-Analysis of Treatment Effects of Randomized Controlled Trials
Abstract
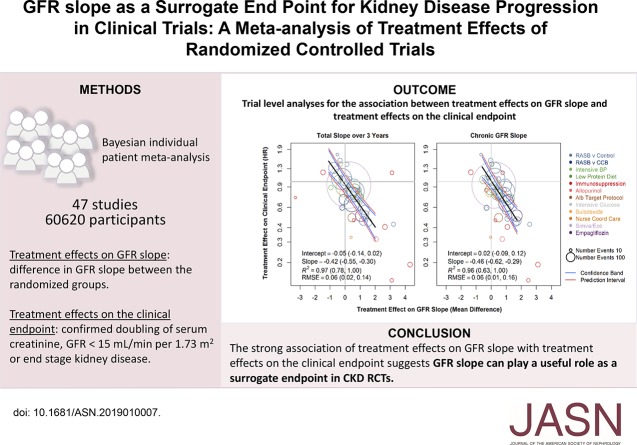
Background: Surrogate end points are needed to assess whether treatments are effective in the early stages of CKD. GFR decline leads to kidney failure, but regulators have not approved using differences in the change in GFR from the beginning to the end of a randomized, controlled trial as an end point in CKD because it is not clear whether small changes in the GFR slope will translate to clinical benefits.
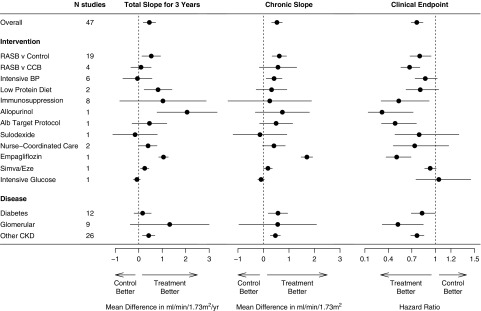
Methods: To assess the use of GFR slope as a surrogate end point for CKD progression, we performed a meta-analysis of 47 RCTs that tested 12 interventions in 60,620 subjects. We estimated treatment effects on GFR slope (mean difference in GFR slope between the randomized groups), for the total slope starting at baseline, chronic slope starting at 3 months after randomization, and on the clinical end point (doubling of serum creatinine, GFR<15 ml/min per 1.73 m2, or ESKD) for each study. We used Bayesian mixed-effects analyses to describe the association of treatment effects on GFR slope with the clinical end point and to test how well the GFR slope predicts a treatment's effect on the clinical end point.
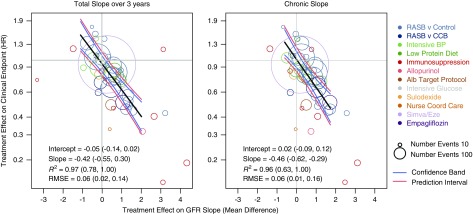
Results: Across all studies, the treatment effect on 3-year total GFR slope (median R2=0.97; 95% Bayesian credible interval [BCI], 0.78 to 1.00) and on the chronic slope (R2 0.96; 95% BCI, 0.63 to 1.00) accurately predicted treatment effects on the clinical end point. With a sufficient sample size, a treatment effect of 0.75 ml/min per 1.73 m2/yr or greater on total slope over 3 years or chronic slope predicts a clinical benefit on CKD progress with at least 96% probability.
Conclusions: With large enough sample sizes, GFR slope may be a viable surrogate for clinical end points in CKD RCTs.
Keywords: GFR; chronic kidney disease; end stage kidney disease; meta-analysis; randomized controlled trials.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
-
Clinical Trial Data Sharing: The Time Is Now.J Am Soc Nephrol. 2019 Sep;30(9):1556-1558. doi: 10.1681/ASN.2019070731. Epub 2019 Aug 13. J Am Soc Nephrol. 2019. PMID: 31409728 Free PMC article. No abstract available.
References
-
- Levey AS, Coresh J: Chronic kidney disease. Lancet 379: 165–180, 2012 - PubMed
-
- Levey AS, Inker LA, Matsushita K, Greene T, Willis K, Lewis E, et al. : GFR decline as an end point for clinical trials in CKD: A scientific workshop sponsored by the national kidney foundation and the US Food and drug administration. Am J Kidney Dis 64: 821–835, 2014 - PubMed
-
- Schievink B, Kröpelin T, Mulder S, Parving HH, Remuzzi G, Dwyer J, et al. : Early renin-angiotensin system intervention is more beneficial than late intervention in delaying end-stage renal disease in patients with type 2 diabetes. Diabetes Obes Metab 18: 64–71, 2016 - PubMed
-
- Matsushita K, Coresh J, Sang Y, Chalmers J, Fox C, Guallar E, et al. ; CKD Prognosis Consortium: Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: A collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol 3: 514–525, 2015 - PMC - PubMed
-
- Astor BC, Matsushita K, Gansevoort RT, van der Velde M, Woodward M, Levey AS, et al. ; Chronic Kidney Disease Prognosis Consortium: Lower estimated glomerular filtration rate and higher albuminuria are associated with mortality and end-stage renal disease. A collaborative meta-analysis of kidney disease population cohorts. Kidney Int 79: 1331–1340, 2011 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
