

Evaluating Glomerular Filtration Rate Slope as a Surrogate End Point for ESKD in Clinical Trials: An Individual Participant Meta-Analysis of Observational Data
- PMID: 31292199
- PMCID: PMC6727262
- DOI: 10.1681/ASN.2019010008
Evaluating Glomerular Filtration Rate Slope as a Surrogate End Point for ESKD in Clinical Trials: An Individual Participant Meta-Analysis of Observational Data
Abstract
Background: Decline in eGFR is a biologically plausible surrogate end point for the progression of CKD in clinical trials. However, it must first be tested to ensure strong associations with clinical outcomes in diverse populations, including patients with higher eGFR.
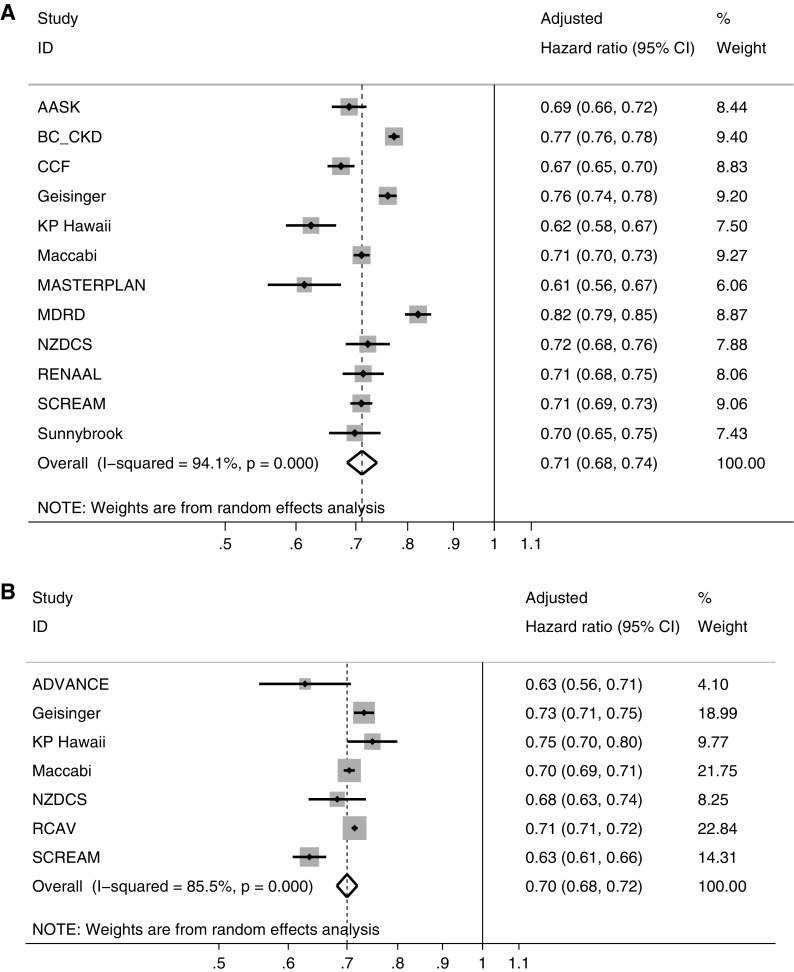
Methods: To investigate the association between 1-, 2-, and 3-year changes in eGFR (slope) with clinical outcomes over the long term, we conducted a random effects meta-analysis of 3,758,551 participants with baseline eGFR≥60 ml/min per 1.73 m2 and 122,664 participants with eGFR<60 ml/min per 1.73 m2 from 14 cohorts followed for an average of 4.2 years.
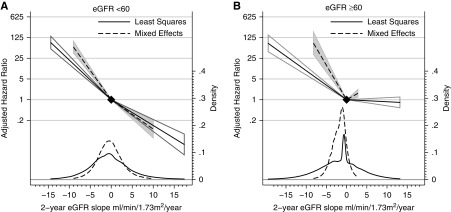
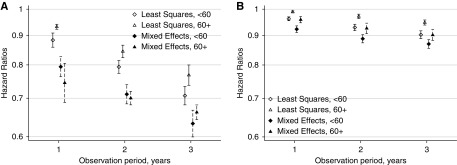
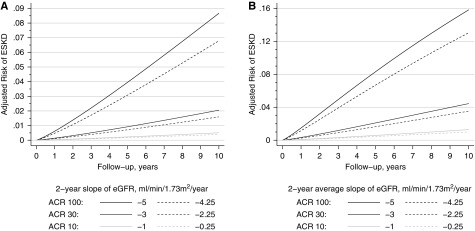
Results: Slower eGFR decline by 0.75 ml/min per 1.73 m2 per year over 2 years was associated with lower risk of ESKD in participants with baseline eGFR≥60 ml/min per 1.73 m2 (adjusted hazard ratio, 0.70; 95% CI, 0.68 to 0.72) and eGFR<60 ml/min per 1.73 m2 (0.71; 95% CI, 0.68 to 0.74). The relationship was stronger with 3-year slope. For a rapidly progressing population with predicted 5-year risk of ESKD of 8.3%, an intervention that reduced eGFR decline by 0.75 ml/min per 1.73 m2 per year over 2 years would reduce the ESKD risk by 1.6%. For a hypothetical low-risk population with a predicted 5-year ESKD risk of 0.58%, the same intervention would reduce the risk by only 0.13%.
Conclusions: Slower decline in eGFR was associated with lower risk of subsequent ESKD, even in participants with eGFR≥60 ml/min per 1.73 m2, but those with the highest risk would be expected to benefit the most.
Keywords: chronic kidney disease; end-stage renal disease; glomerular filtration rate; progression of chronic renal failure.
Copyright © 2019 by the American Society of Nephrology.
Figures
References
-
- Himmelfarb J: Chronic kidney disease and the public health: Gaps in evidence from interventional trials. JAMA 297: 2630–2633, 2007 - PubMed
-
- Strippoli GF, Craig JC, Schena FP: The number, quality, and coverage of randomized controlled trials in nephrology. J Am Soc Nephrol 15: 411–419, 2004 - PubMed
-
- Thompson A, Lawrence J, Stockbridge N: GFR decline as an end point in trials of CKD: A viewpoint from the FDA. Am J Kidney Dis 64: 836–837, 2014 - PubMed
-
- Inker LA, Mondal H, Greene T, Masaschi T, Locatelli F, Schena FP, et al. .: Early change in urine protein as a surrogate end point in studies of IgA nephropathy: An individual-patient meta-analysis. Am J Kidney Dis 68: 392–401, 2016 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
