

Cumulative Antibiotic Use Significantly Decreases Efficacy of Checkpoint Inhibitors in Patients with Advanced Cancer
- PMID: 31292268
- PMCID: PMC6964118
- DOI: 10.1634/theoncologist.2019-0160
Cumulative Antibiotic Use Significantly Decreases Efficacy of Checkpoint Inhibitors in Patients with Advanced Cancer
Abstract
Background: With the advent of immunotherapy, substantial progress has been made in improving outcomes for patients with advanced cancer. However, not all patients benefit equally from treatment, and confounding immune-related issues may have an impact. Several studies suggest that antibiotic use (which alters the gut microbiome) may result in poorer outcomes for patients treated with immune checkpoint inhibitors (ICI).
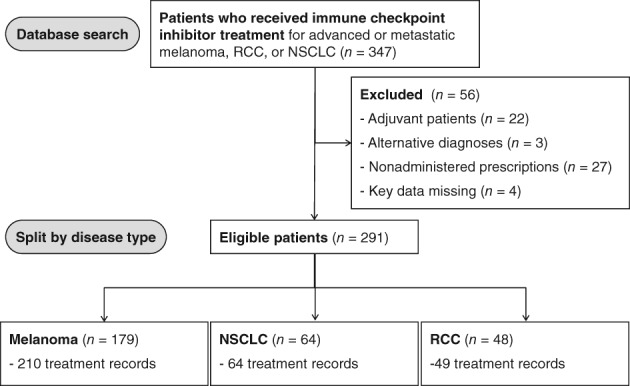
Materials and methods: This is a large, single-site retrospective review of n = 291 patients with advanced cancer treated with ICI (n = 179 melanoma, n = 64 non-small cell lung cancer, and n = 48 renal cell carcinoma). Antibiotic use (both single and multiple courses/prolonged use) during the periods 2 weeks before and 6 weeks after ICI treatment was investigated.
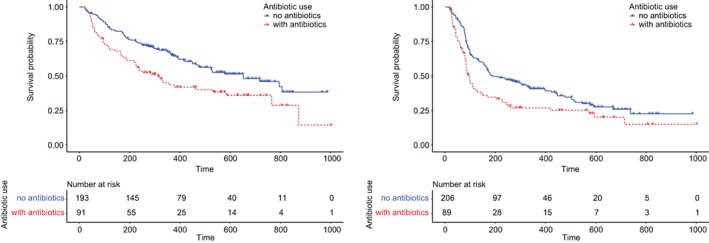
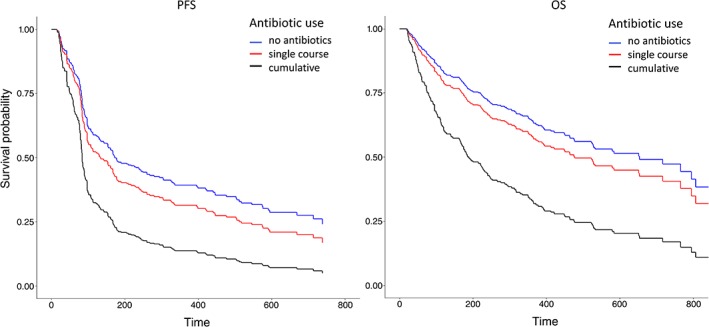
Results: Within this cohort, 92 patients (32%) received antibiotics. Patients who did not require antibiotics had the longest median progression-free survival (PFS), of 6.3 months, and longest median overall survival (OS), of 21.7 months. With other clinically relevant factors controlled, patients who received a single course of antibiotics had a shorter median OS (median OS, 17.7 months; p = .294), and patients who received multiple courses or prolonged antibiotic treatment had the worst outcomes overall (median OS, 6.3 months; p = .009). Progression-free survival times were similarly affected.
Conclusion: This large, multivariate analysis demonstrated that antibiotic use is an independent negative predictor of PFS and OS in patients with advanced cancer treated with ICIs. This study highlighted worse treatment outcomes from patients with cumulative (multiple or prolonged courses) antibiotic use, which warrants further investigation and may subsequently inform clinical practice guidelines advocating careful use of antibiotics.
Implications for practice: Antibiotic use is negatively associated with treatment outcomes of immune checkpoint inhibitors (ICI) in advanced cancer. Cumulative antibiotic use is associated with a marked negative survival outcome. Judicious antibiotic prescribing is warranted in patients receiving treatment with ICI for treatment of advanced malignancy.
Keywords: Checkpoint inhibitors; Cumulative antibiotics; Immunotherapy; Lung cancer; Melanoma; Renal cancer.
© AlphaMed Press 2019.
Figures
Comment in
-
Gut microbiome, antibiotic use, and immunotherapy responsiveness in cancer.Ann Transl Med. 2019 Dec;7(Suppl 8):S309. doi: 10.21037/atm.2019.10.27. Ann Transl Med. 2019. PMID: 32016028 Free PMC article. No abstract available.
-
Immune-checkpoint inhibitors and the importance of concomitant medications: focus on antibiotics.Ann Transl Med. 2019 Dec;7(Suppl 8):S339. doi: 10.21037/atm.2019.09.99. Ann Transl Med. 2019. PMID: 32016057 Free PMC article. No abstract available.
References
-
- Blank CU, Haanen JB, Ribas A et al. Cancer immunology. The “cancer immunogram.” Science 2016;352:658–660. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
