

Decreased maternal serum acetate and impaired fetal thymic and regulatory T cell development in preeclampsia
- PMID: 31292453
- PMCID: PMC6620275
- DOI: 10.1038/s41467-019-10703-1
Decreased maternal serum acetate and impaired fetal thymic and regulatory T cell development in preeclampsia
Abstract
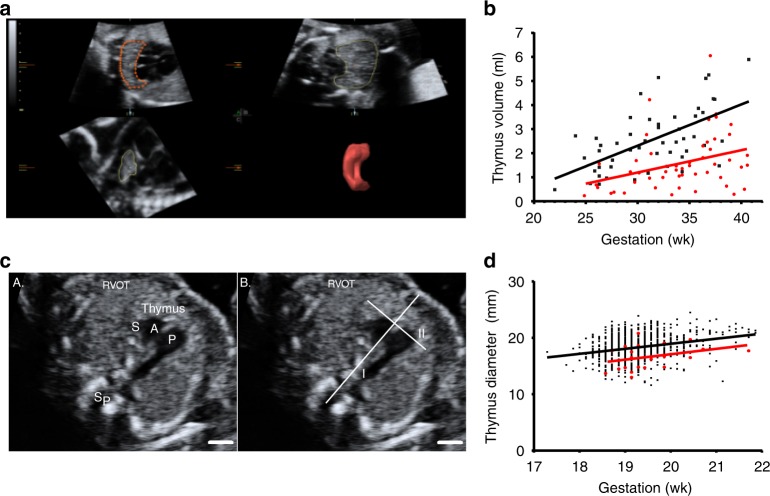
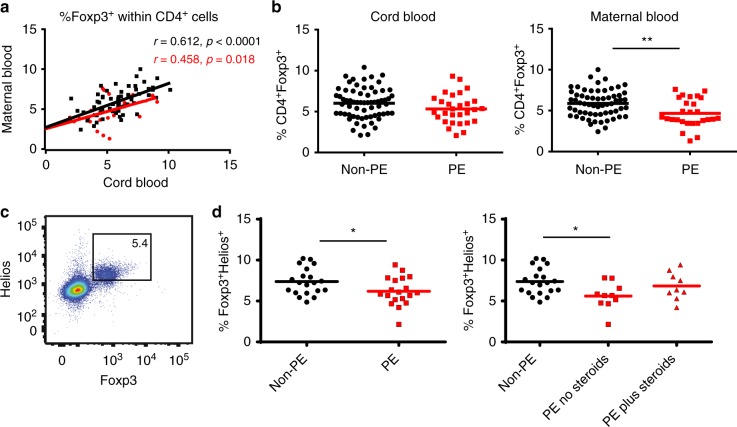
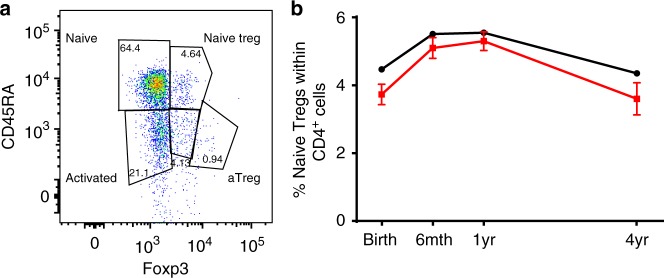
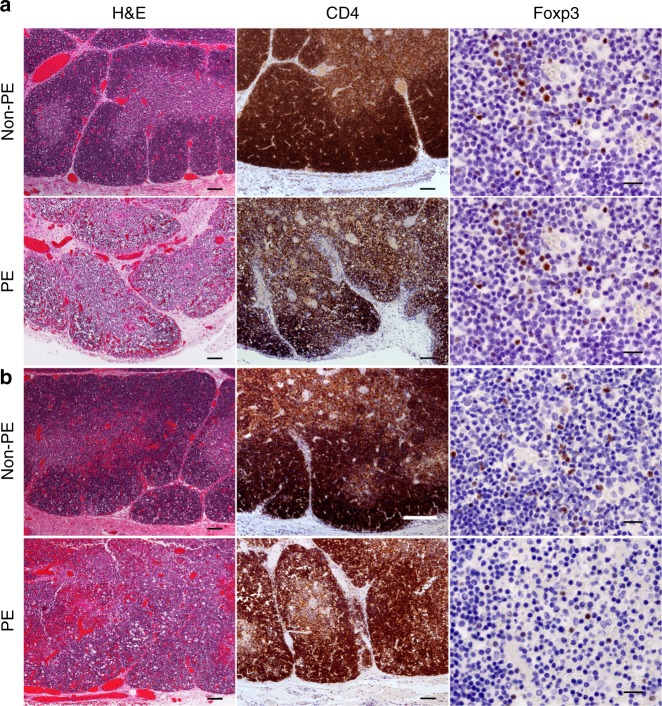
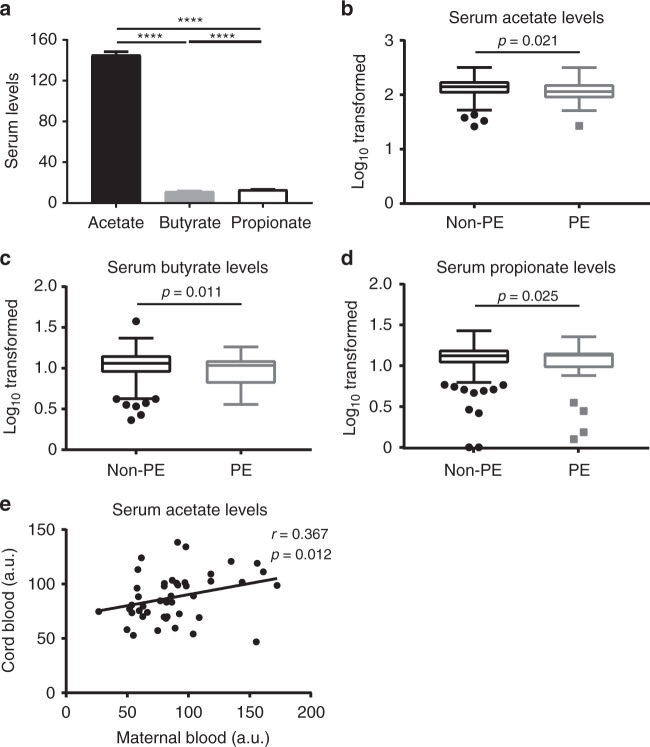
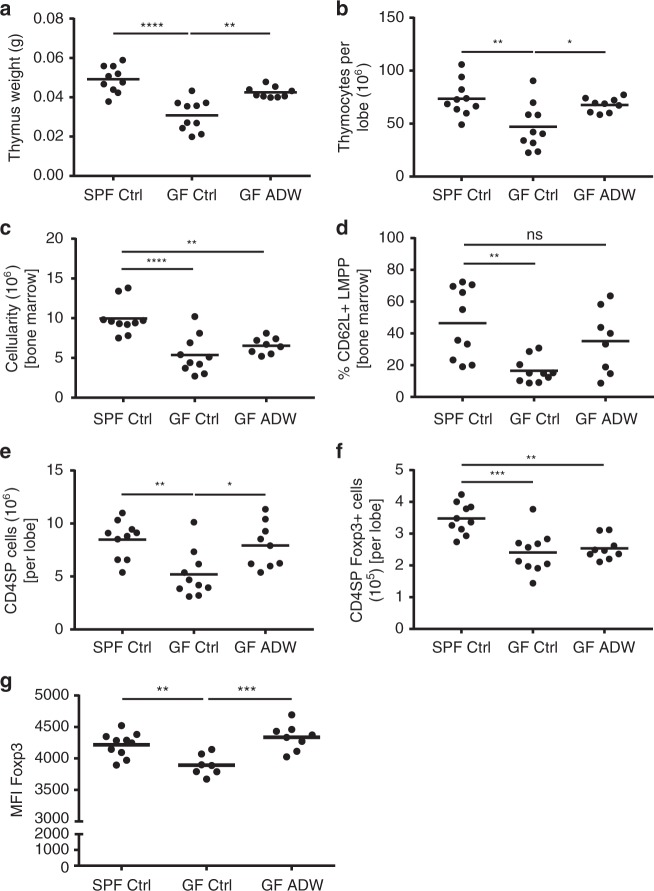
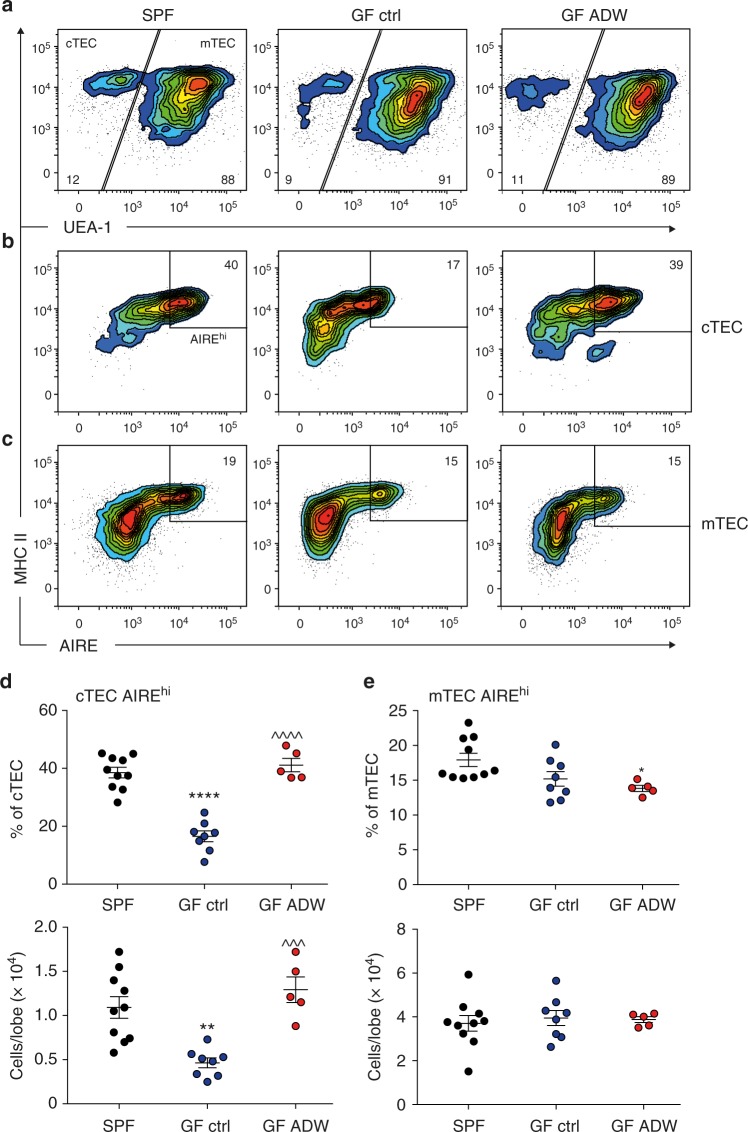
Maternal immune dysregulation seems to affect fetal or postnatal immune development. Preeclampsia is a pregnancy-associated disorder with an immune basis and is linked to atopic disorders in offspring. Here we show reduction of fetal thymic size, altered thymic architecture and reduced fetal thymic regulatory T (Treg) cell output in preeclamptic pregnancies, which persists up to 4 years of age in human offspring. In germ-free mice, fetal thymic CD4+ T cell and Treg cell development are compromised, but rescued by maternal supplementation with the intestinal bacterial metabolite short chain fatty acid (SCFA) acetate, which induces upregulation of the autoimmune regulator (AIRE), known to contribute to Treg cell generation. In our human cohorts, low maternal serum acetate is associated with subsequent preeclampsia, and correlates with serum acetate in the fetus. These findings suggest a potential role of acetate in the pathogenesis of preeclampsia and immune development in offspring.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Bacterial metabolites shape neonatal immune system.Nat Rev Immunol. 2019 Sep;19(9):537. doi: 10.1038/s41577-019-0207-7. Nat Rev Immunol. 2019. PMID: 31371823 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
