

New therapeutic target for pediatric anaplastic ependymoma control: study of anti-tumor activity by a Kunitz-type molecule, Amblyomin-X
- PMID: 31292491
- PMCID: PMC6620274
- DOI: 10.1038/s41598-019-45799-4
New therapeutic target for pediatric anaplastic ependymoma control: study of anti-tumor activity by a Kunitz-type molecule, Amblyomin-X
Abstract
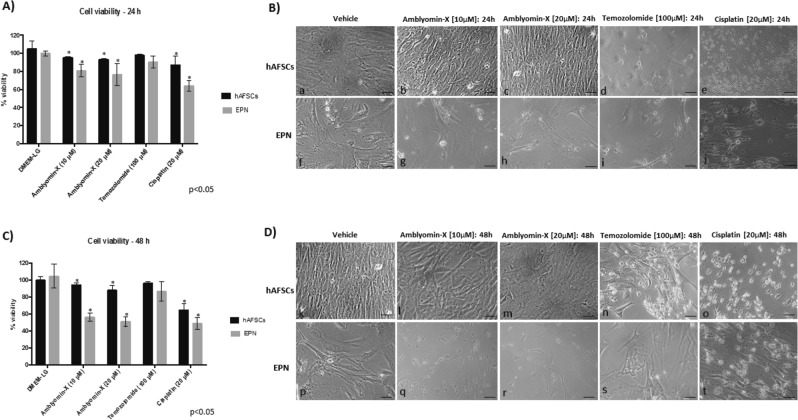
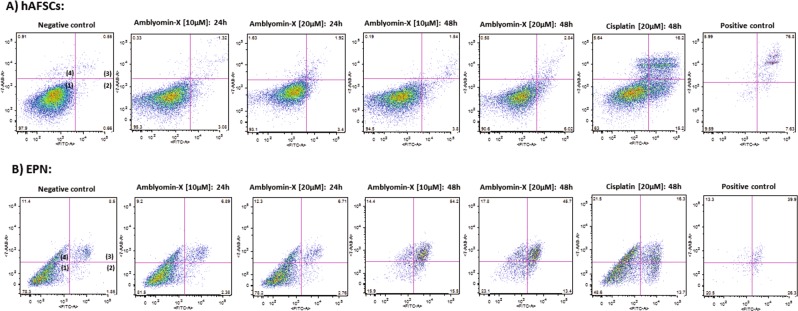
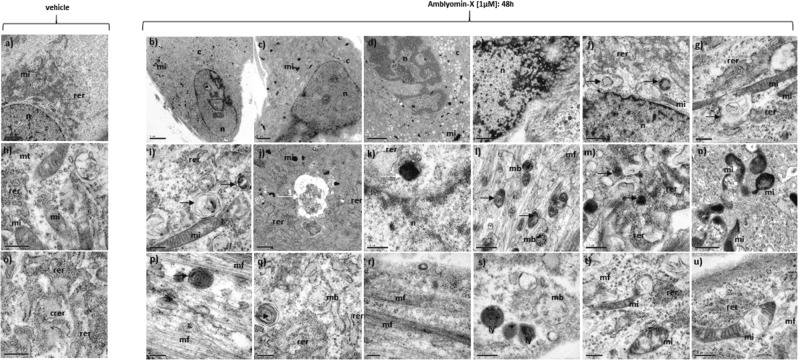
EPNs comprise a heterogeneous group of neuroepithelial tumors, accounting for about 10% of all intracranial tumors in children and up to 30% of brain tumors in those younger than 3 years. Actually, the pattern therapy for low-grade EPNs includes complete surgical resection followed by radiation therapy. Total surgical excision is often not possible due to tumor location. The aim of this study was to evaluate, for the first time, the anti-tumor activity of Amblyomin-X in 4 primary cultures derived from pediatric anaplastic posterior fossa EPN, Group A (anaplastic, WHO grade III) and one primary culture of a high grade neuroepithelial tumor with MN1 alteration, which was initially misdiagnosed as EPN: i) by in vitro assays: comparisons of temozolomide and cisplatin; ii) by intracranial xenograft model. Amblyomin-X was able to induce cell death in EPN cells in a more significant percentage compared to cisplatin. The cytotoxic effects of Amblyomin-X were not detected on hFSCs used as control, as opposed to cisplatin-treatment, which promoted a substantial effect in the hAFSCs viability. TEM analysis showed ultrastructural alterations related to the process of cell death: mitochondrial degeneration, autophagosomes and aggregate-like structures. MRI and histopathological analyzes demonstrated significant tumor mass regression. Our results suggest that Amblyomin-X has a selective effect on tumor cells by inducing apoptotic cell death and may be a therapeutic option for Group AEPNs.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Ostrom Quinn T., Gittleman Haley, Fulop Jordonna, Liu Max, Blanda Rachel, Kromer Courtney, Wolinsky Yingli, Kruchko Carol, Barnholtz-Sloan Jill S. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2008-2012. Neuro-Oncology. 2015;17(suppl 4):iv1–iv62. doi: 10.1093/neuonc/nov189. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
