

Real-World Data on Prognostic Factors for Overall Survival in EGFR-Mutant Non-Small-Cell Lung Cancer Patients with Brain Metastases
- PMID: 31293653
- PMCID: PMC6603428
- DOI: 10.7150/jca.30292
Real-World Data on Prognostic Factors for Overall Survival in EGFR-Mutant Non-Small-Cell Lung Cancer Patients with Brain Metastases
Abstract
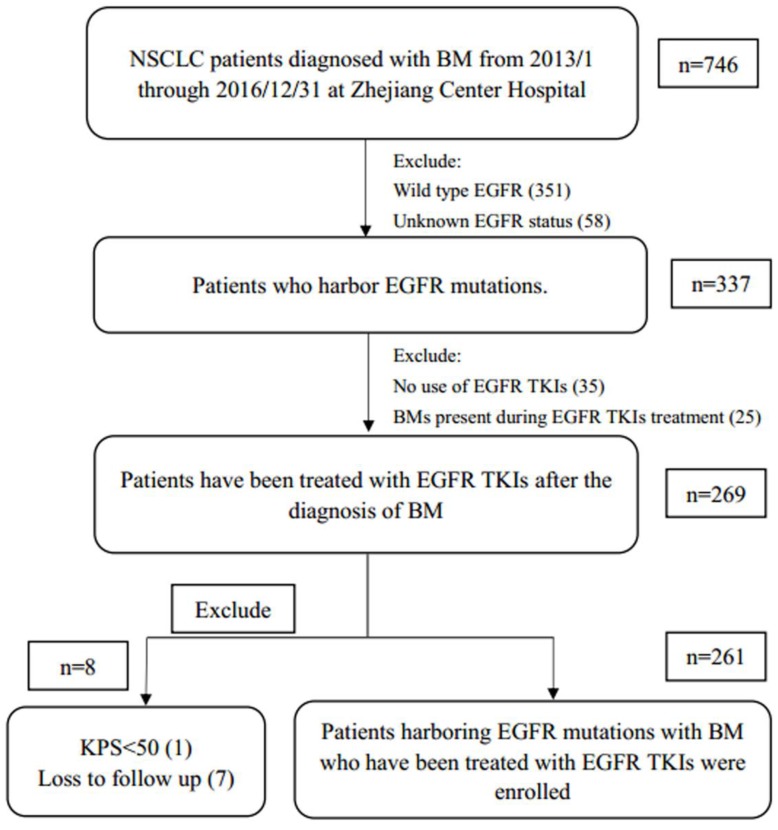
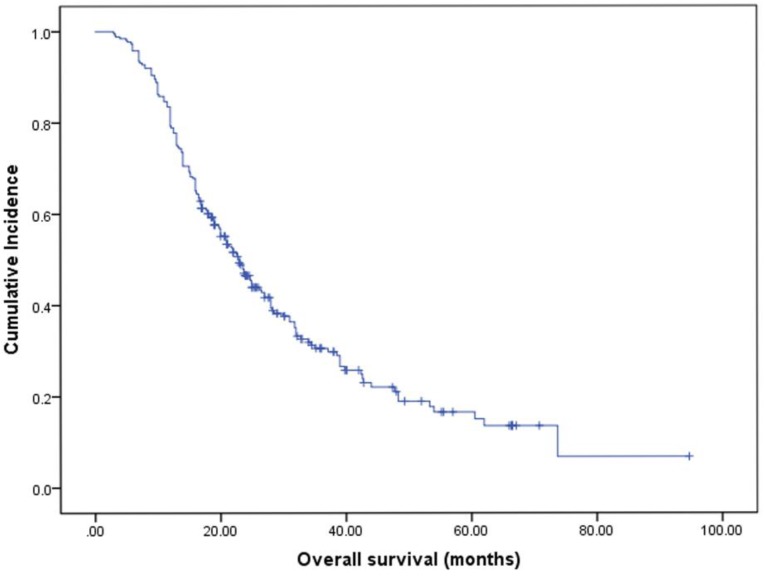
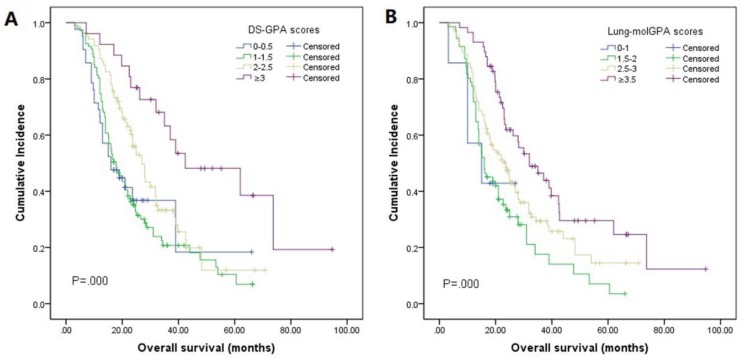
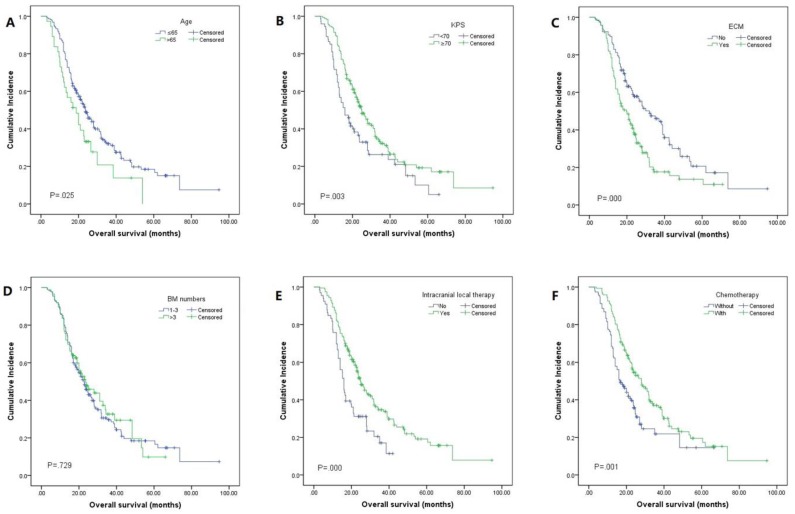
Background: With the wide application of epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs), the survival of EGFR-mutant non-small-cell lung cancer (NSCLC) patients with brain metastasis (BM) has been significantly improved. However, prognosis analysis for patients with EGFR mutation and BM is still lacking, and the prognostic factors remain to be determined. Materials and methods: A total of 746 NSCLC patients with BM were identified between January 2013 and December 2016 at our institution. Overall, 261 patients harboring EGFR mutation and meeting the inclusion criteria for the study were enrolled. Exclusion criteria included KPS<50, diagnosed with BM during treatment with EGFR-TKIs, or insufficient follow-up. Overall survival (OS) was measured from the date of brain metastases. Independent prognostic factors were confirmed using a Cox regression model. Results: The median follow-up time for these patients was 32.7 months (95% CI, 23.5-41.9). The median OS after development of brain metastases was 23.0 months (95% CI, 20.01-25.99). By univariate analysis, significantly shorter OS was noted in patients older than 65 years (p=0.025), KPS <70 (p=0.003), presence of extracranial metastases (ECM) (p=0.00), without intracranial local treatment (p=0.000), and without chemotherapy (p=0.001). There was no difference in OS with respect to EGFR mutation type and number of BM (p=0.343, p=0.729, respectively). The Cox proportional hazards regression model revealed that performance status (KPS<70, p=0.010), ECM (p=0.001), receiving intracranial local treatment (p=0.005) and chemotherapy (p=0.005) were independent prognostic factors for OS, while age was not (p=0.087). Patients with higher diagnosis-specific graded prognostic assessment (DS-GPA) and Lung-molGPA scores corresponded to better prognosis (p=0.000). Conclusion: This retrospective analysis demonstrated that performance status (KPS≥70), absence of ECM metastases, administration of local treatment and chemotherapy were associated with superior OS in patients with EGFR-mutant NSCLC who developed BM. The DS-GPA and Lung-molGPA indexes still applied to NSCLC patients with mutant genotypes and BM.
Keywords: Brain Metastases; Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors; Non-Small-Cell Lung Cancer; Prognostic Factors.
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures
References
-
- Dempke WC, Edvardsen K, Lu S, Reinmuth N, Reck M, Inoue A. Brain Metastases in NSCLC - are TKIs Changing the Treatment Strategy? Anticancer Research. 2015;35:5797. - PubMed
-
- Gavrilovic IT, Posner JB. Brain metastases: epidemiology and pathophysiology. Journal of Neuro-Oncology. 2005;75:5–14. - PubMed
-
- H S, L L, T T, M N, M S, II W. et al. Clinical and biological features associated with epidermal growth factor receptor gene mutations in lung cancers. J Natl Cancer Inst. 2005;98:362–3. - PubMed
-
- Magnuson WJ, Lester-Coll NH, Wu AJ, Yang TJ, Lockney NA, Gerber NK. et al. Management of Brain Metastases in Tyrosine Kinase Inhibitor-Naïve Epidermal Growth Factor Receptor-Mutant Non-Small-Cell Lung Cancer: A Retrospective Multi-Institutional Analysis. Journal of Clinical Oncology Official Journal of the American Society of Clinical Oncology. 2017;35:1070. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
