

Hepatocellular carcinoma treatment: hurdles, advances and prospects
- PMID: 31293776
- PMCID: PMC6613045
- DOI: 10.2217/hep-2018-0002
Hepatocellular carcinoma treatment: hurdles, advances and prospects
Abstract
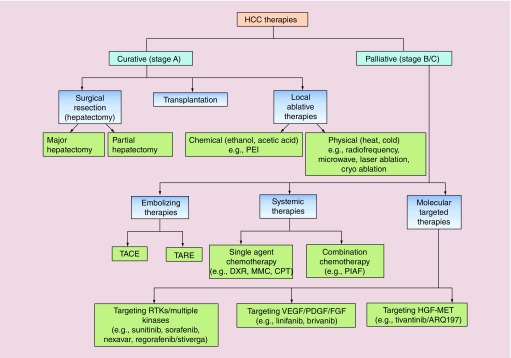
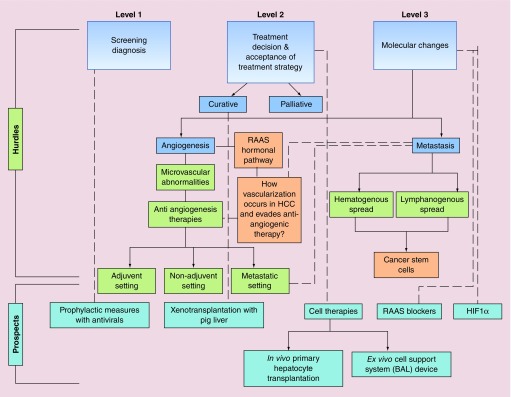
Hepatocellular carcinoma (HCC) is one of the major causes of cancer-related mortality and is particularly refractory to the available chemotherapeutic drugs. Among various etiologies of HCC, viral etiology is the most common, and, along with alcoholic liver disease and nonalcoholic steatohepatitis, accounts for almost 90% of all HCC cases. HCC is a heterogeneous tumor associated with multiple signaling pathway alterations and its complex patho-physiology has made the treatment decision challenging. The potential curative treatment options are effective only in small group of patients, while palliative treatments are associated with improved survival and quality of life for intermediate/advanced stage HCC patients. This review article focuses on the currently available treatment strategies and hurdles encountered for HCC therapy. The curative treatment options discussed are surgical resection, liver transplantation, and local ablative therapies which are effective for early stage HCC patients. The palliative treatment options discussed are embolizing therapies, systemic therapies, and molecular targeted therapies. Besides, the review also focuses on hurdles to be conquered for successful treatment of HCC and specifies the future prospects for HCC treatment. It also discusses the multi-modal approach for HCC management which maximizes the chances of better clinical outcome after treatment and identifies that selection of a particular treatment regimen based on patients' disease stage, patients' ages, and other underlying factors will certainly lead to a better prognosis.
Keywords: Hepatitis; anti-virals; cell-therapies; curative treatment; hepatocellular cracinoma; palliative treatment; regorafenib; sorafenib; transarterial chemoembolization; xenotransplantaion.
Conflict of interest statement
Financial & competing interests disclosure The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. No writing assistance was utilized in the production of this manuscript.
Figures
References
-
- Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: Resection versus transplantation. Hepatology. 1999;30(6):1434–1440. - PubMed
Publication types
LinkOut - more resources
Full Text Sources