

A Model of Pediatric End-Stage Lung Failure in Small Lambs <20 kg
- PMID: 31294720
- PMCID: PMC6851459
- DOI: 10.1097/MAT.0000000000001017
A Model of Pediatric End-Stage Lung Failure in Small Lambs <20 kg
Abstract
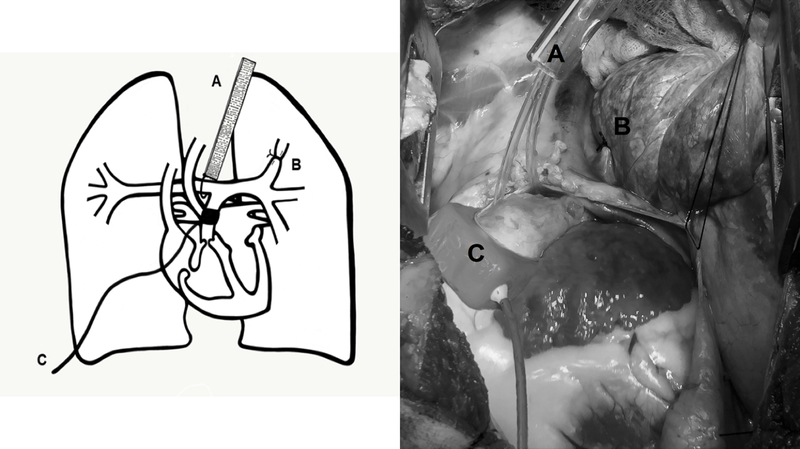
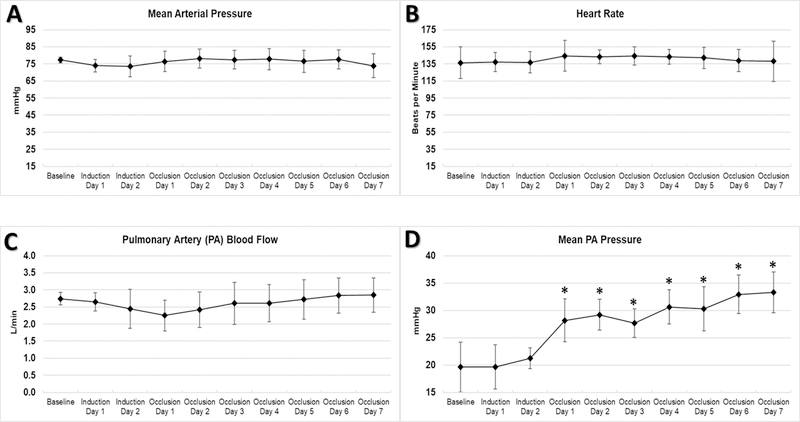
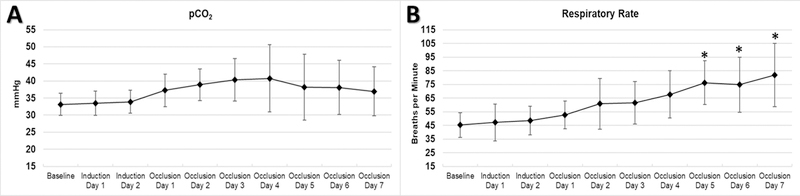
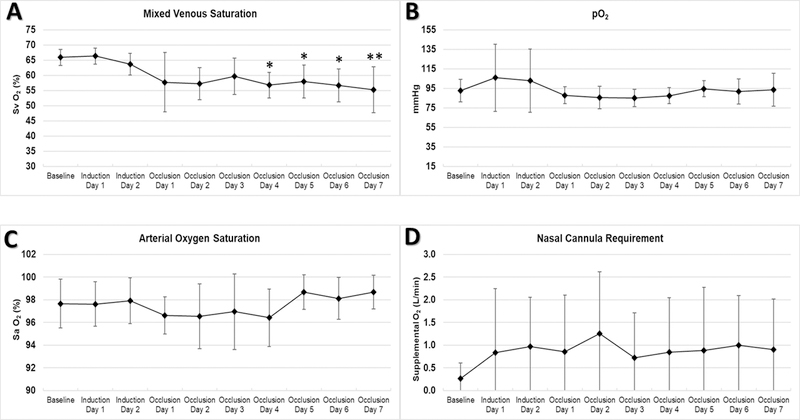
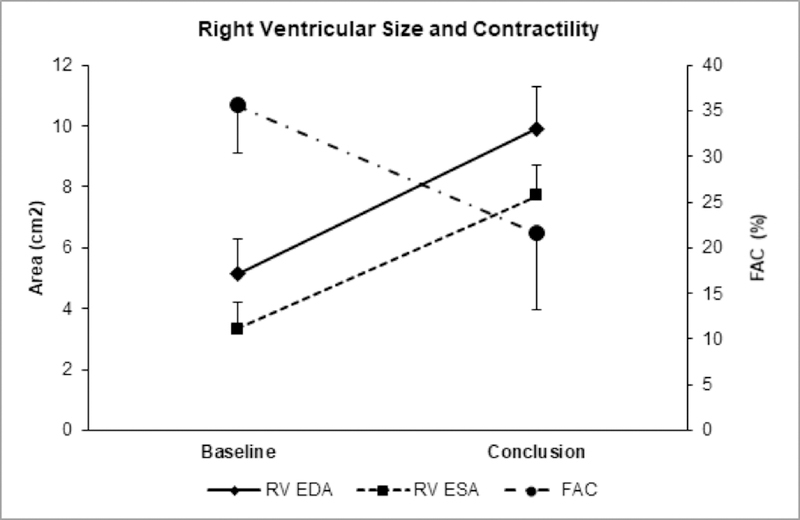
One in five children with end-stage lung failure (ESLF) die while awaiting lung transplant. No suitable animal model of ESLF exists for the development of artificial lung devices for bridging to transplant. Small lambs weighing 15.7 ± 3.1 kg (n = 5) underwent ligation of the left anterior pulmonary artery (PA) branch, and gradual occlusion of the right main PA over 48 hours. All animals remained hemodynamically stable. Over seven days of disease model conditions, they developed pulmonary hypertension (mean PA pressure 20 ± 5 vs. 33 ± 4 mm Hg), decreased perfusion (SvO2 66 ± 3 vs. 55 ± 8%) with supplemental oxygen requirement, and severe tachypneic response (45 ± 9 vs. 82 ± 23 breaths/min) (all p < 0.05). Severe right heart dysfunction developed (tricuspid annular plane systolic excursion 13 ± 3 vs. 7 ± 2 mm, fractional area change 36 ± 6 vs. 22 ± 10 mm, ejection fraction 51 ± 9 vs. 27 ± 17%, all p < 0.05) with severe tricuspid regurgitation and balloon-shaped dilation of the right ventricle. This model of pediatric ESLF reliably produces pulmonary hypertension, right heart strain, and impaired gas exchange, and will be used to develop a pediatric artificial lung.
Conflict of interest statement
CONFLICTS OF INTEREST:
The authors have no conflicts of interest to disclose.
Figures

References
-
- Valapour M, Skeans MA, Smith JM, et al. : OPTN/SRTR 2015 Annual Data Report: Lung. Am J Transplant 17 Suppl 1: 357–424, 2017. - PubMed
-
- Zwischenberger JB, Anderson CM, Cook KE, Lick SD, Mockros LF, Bartlett RH: Development of an implantable artificial lung: challenges and progress. ASAIO J 47 (4): 316–20, 2001. - PubMed
-
- Skinner SC, Hirschl RB, Bartlett RH: Extracorporeal life support. Semin Pediatr Surg 15 (4): 242–50, 2006. - PubMed
-
- Bartlett RH, Deatrick KB: Current and future status of extracorporeal life support for respiratory failure in adults. Curr Opin Crit Care 22 (1): 80–5, 2016. - PubMed
-
- Griffith BP: Children are not necessarily “small” adults: the growing field of miniaturized mechanical circulatory support. J Heart Lung Transplant 30 (1): 9–11, 2011. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
