

Canadian Association of Gastroenterology Clinical Practice Guideline for the Management of Irritable Bowel Syndrome (IBS)
- PMID: 31294724
- PMCID: PMC6507291
- DOI: 10.1093/jcag/gwy071
Canadian Association of Gastroenterology Clinical Practice Guideline for the Management of Irritable Bowel Syndrome (IBS)
Abstract
Background & aims: Irritable bowel syndrome (IBS) is one of the most common gastrointestinal (GI) disorders, affecting about 10% of the general population globally. The aim of this consensus was to develop guidelines for the management of IBS.
Methods: A systematic literature search identified studies on the management of IBS. The quality of evidence and strength of recommendations were rated according to the Grading of Recommendation Assessment, Development and Evaluation (GRADE) approach. Statements were developed through an iterative online platform and then finalized and voted on by a multidisciplinary group of clinicians and a patient.
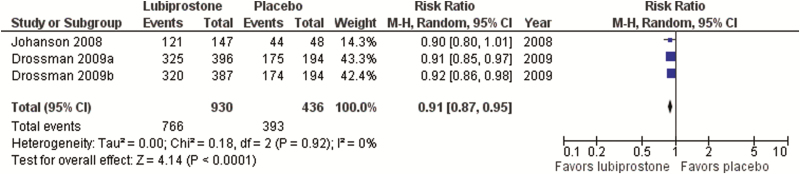
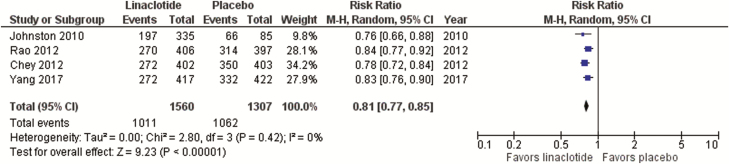
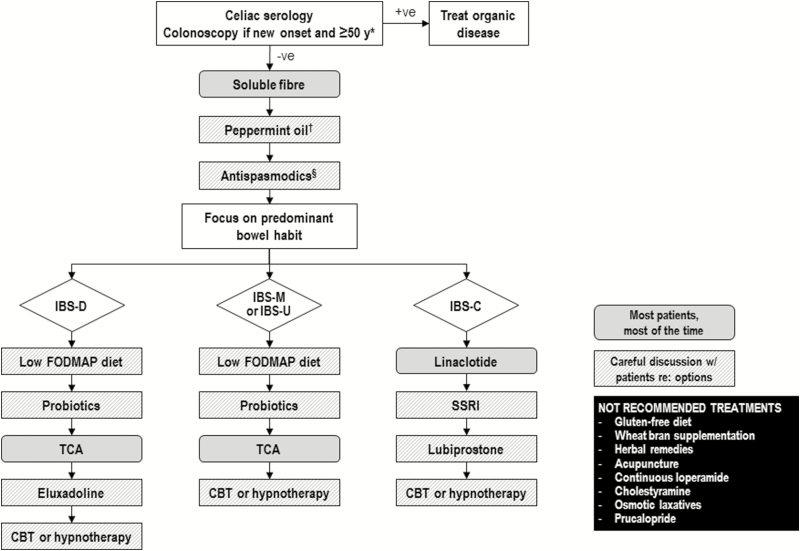
Results: Consensus was reached on 28 of 31 statements. Irritable bowel syndrome is diagnosed based on symptoms; serological testing is suggested to exclude celiac disease, but routine testing for C-reactive protein (CRP), fecal calprotectin or food allergies is not recommended. A trial of a low fermentable oligosaccharides, disaccharides, monosaccharides, polyols (FODMAP) diet is suggested, while a gluten-free diet is not. Psyllium, but not wheat bran, supplementation may help reduce symptoms. Alternative therapies such as peppermint oil and probiotics are suggested, while herbal therapies and acupuncture are not. Cognitive behavioural therapy and hypnotherapy are suggested psychological therapies. Among the suggested or recommended pharmacological therapies are antispasmodics, certain antidepressants, eluxadoline, lubiprostone, and linaclotide. Loperamide, cholestyramine and osmotic laxatives are not recommended for overall IBS symptoms. The nature of the IBS symptoms (diarrhea-predominant or constipation-predominant) should be considered in the choice of pharmacological treatments.
Conclusions: Patients with IBS may benefit from a multipronged, individualized approach to treatment, including dietary modifications, psychological and pharmacological therapies.
Keywords: Clinical practice guidelines; Constipation; Diarrhea; Irritable bowel syndrome.
Figures

References
-
- Lacy BE, Mearin F, Chang L, et al. Bowel disorders. Gastroenterology 2016;150:1393–407.e5. - PubMed
-
- Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: A meta-analysis. Clin Gastroenterol Hepatol 2012;10(7):712–721.e4. - PubMed
-
- Sperber AD, Dumitrascu D, Fukudo S, et al. The global prevalence of IBS in adults remains elusive due to the heterogeneity of studies: A Rome Foundation working team literature review. Gut 2017;66(6):1075–82. - PubMed
-
- Thompson WG, Irvine EJ, Pare P, et al. Functional gastrointestinal disorders in Canada: First population-based survey using Rome II criteria with suggestions for improving the questionnaire. Dig Dis Sci 2002;47(1):225–35. - PubMed
-
- Palsson OS, van Tilburg MA, Simren M, et al. Population prevalence of Rome IV and Rome III irritable bowel syndrome (IBS) in the United States (US), Canada and the United Kingdom (UK) [Abstract Mo1642]. Gastroenterology 2016;150:S739–40.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous