

Identifying determinants of persistent MRSA bacteremia using mathematical modeling
- PMID: 31295255
- PMCID: PMC6622483
- DOI: 10.1371/journal.pcbi.1007087
Identifying determinants of persistent MRSA bacteremia using mathematical modeling
Abstract
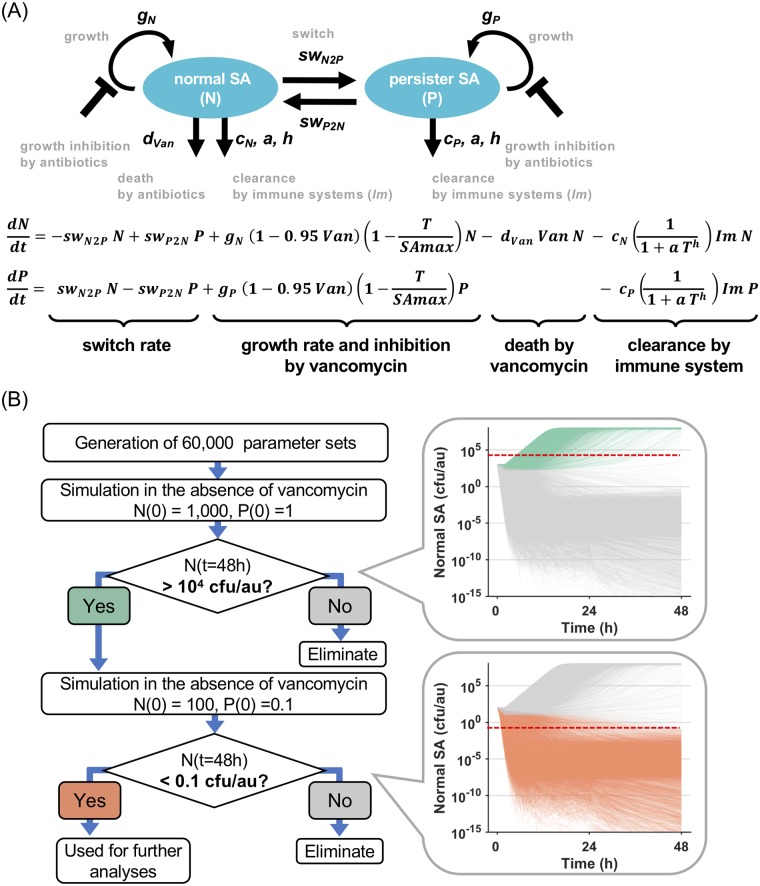
Persistent bacteremia caused by Staphylococcus aureus (SA), especially methicillin-resistant SA (MRSA), is a significant cause of morbidity and mortality. Despite susceptibility phenotypes in vitro, persistent MRSA strains fail to clear with appropriate anti-MRSA therapy during bacteremia in vivo. Thus, identifying the factors that cause such MRSA persistence is of direct and urgent clinical relevance. To address the dynamics of MRSA persistence in the face of host immunity and typical antibiotic regimens, we developed a mathematical model based on the overarching assumption that phenotypic heterogeneity is a hallmark of MRSA persistence. First, we applied an ensemble modeling approach and obtained parameter sets that satisfied the condition of a minimum inoculum dose to establish infection. Second, by simulating with the selected parameter sets under vancomycin therapy which follows clinical practices, we distinguished the models resulting in resolving or persistent bacteremia, based on the total SA exceeding a detection limit after five days of treatment. Third, to find key determinants that discriminate resolving and persistent bacteremia, we applied a machine learning approach and found that the immune clearance rate of persister cells is a key feature. But, fourth, when relapsing bacteremia was considered, the growth rate of persister cells was also found to be a key feature. Finally, we explored pharmacological strategies for persistent and relapsing bacteremia and found that a persister killer, but not a persister formation inhibitor, could provide for an effective cure the persistent bacteremia. Thus, to develop better clinical solutions for MRSA persistence and relapse, our modeling results indicate that we need to better understand the pathogen-host interactions of persister MRSAs in vivo.
Conflict of interest statement
MRY is founder and shareholder of NovaDigm Therapeutics, Inc. which develops vaccines and immunotherapeutics for infections, including Staphylococcus aureus.
Figures






Similar articles
-
Methicillin-resistant Staphylococcus aureus bacteremia in hemodialysis and nondialysis patients.J Microbiol Immunol Infect. 2014 Feb;47(1):15-22. doi: 10.1016/j.jmii.2012.08.015. Epub 2012 Oct 3. J Microbiol Immunol Infect. 2014. PMID: 23040238
-
[Evaluation of methicillin-resistant Staphylococcus aureus bacteremia and comparison of prognosis according to vancomycin MIC values: experience of the last ten years].Mikrobiyol Bul. 2013 Apr;47(2):199-210. doi: 10.5578/mb.4530. Mikrobiyol Bul. 2013. PMID: 23621720 Turkish.
-
Methicillin-resistant Staphylococcus aureus (MRSA) staphylococcal cassette chromosome mec genotype effects outcomes of patients with healthcare-associated MRSA bacteremia independently of vancomycin minimum inhibitory concentration.Clin Infect Dis. 2012 Nov 15;55(10):1329-37. doi: 10.1093/cid/cis717. Epub 2012 Aug 20. Clin Infect Dis. 2012. PMID: 22911641
-
Bacteremia due to Methicillin-Resistant Staphylococcus aureus: New Therapeutic Approaches.Infect Dis Clin North Am. 2016 Jun;30(2):491-507. doi: 10.1016/j.idc.2016.02.009. Infect Dis Clin North Am. 2016. PMID: 27208769 Review.
-
[Consensus document for the treatment of bacteremia and endocarditis caused by methicillin-resistent Staphylococcus aureus. Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica].Enferm Infecc Microbiol Clin. 2009 Feb;27(2):105-15. doi: 10.1016/j.eimc.2008.09.003. Epub 2009 Feb 11. Enferm Infecc Microbiol Clin. 2009. PMID: 19254641 Review. Spanish.
Cited by
-
Topical Nanotherapeutics for Treating MRSA-Associated Skin and Soft Tissue Infection (SSTIs).AAPS PharmSciTech. 2023 Apr 26;24(5):108. doi: 10.1208/s12249-023-02563-2. AAPS PharmSciTech. 2023. PMID: 37100956 Review.
-
Hospital Acquired Sepsis, Disease Prevalence, and Recent Advances in Sepsis Mitigation.Pathogens. 2024 May 30;13(6):461. doi: 10.3390/pathogens13060461. Pathogens. 2024. PMID: 38921759 Free PMC article. Review.
-
Computational and in vitro evaluation of probiotic treatments for nasal Staphylococcus aureus decolonization.Proc Natl Acad Sci U S A. 2025 Feb 18;122(7):e2412742122. doi: 10.1073/pnas.2412742122. Epub 2025 Feb 11. Proc Natl Acad Sci U S A. 2025. PMID: 39932999 Free PMC article.
-
Anti-MRSA agent discovery using Caenorhabditis elegans-based high-throughput screening.J Microbiol. 2020 Jun;58(6):431-444. doi: 10.1007/s12275-020-0163-8. Epub 2020 May 27. J Microbiol. 2020. PMID: 32462486 Review.
-
Differential effects of antibiotics on neutrophils exposed to lipoteichoic acid derived from Staphylococcus aureus.Ann Clin Microbiol Antimicrob. 2020 Nov 3;19(1):50. doi: 10.1186/s12941-020-00392-w. Ann Clin Microbiol Antimicrob. 2020. PMID: 33143710 Free PMC article.
References
-
- Chong YP, Park SJ, Kim HS, Kim ES, Kim MN, Park KH, et al. Persistent staphylococcus aureus bacteremia: A prospective analysis of risk factors, outcomes, and microbiologic and genotypic characteristics of isolates. Med (United States). 2013;92: 98–108. 10.1097/MD.0b013e318289ff1e - DOI - PMC - PubMed
